Request Demo
Last update 20 Mar 2025
Lactobacillus plantarum TCI507
Last update 20 Mar 2025
Overview
Basic Info
Drug Type Probiotics |
Synonyms oranges peels Extract, probiotic extracted from the oranges peels |
Target- |
Action modulators |
Mechanism Bacteria replacements, Microbiome modulators |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization- |
Drug Highest PhaseClinical |
First Approval Date- |
Regulation- |

Related
2
Clinical Trials associated with Lactobacillus plantarum TCI507NCT04492605
The Evaluation of TCI378 and TCI507 Probiotics on Weight-lowering Efficacy in Adults
NCT04910620
The Evaluation of TCI378 and TCI507 Probiotics on Weight-lowering Efficacy in Adults
100 Clinical Results associated with Lactobacillus plantarum TCI507
Login to view more data
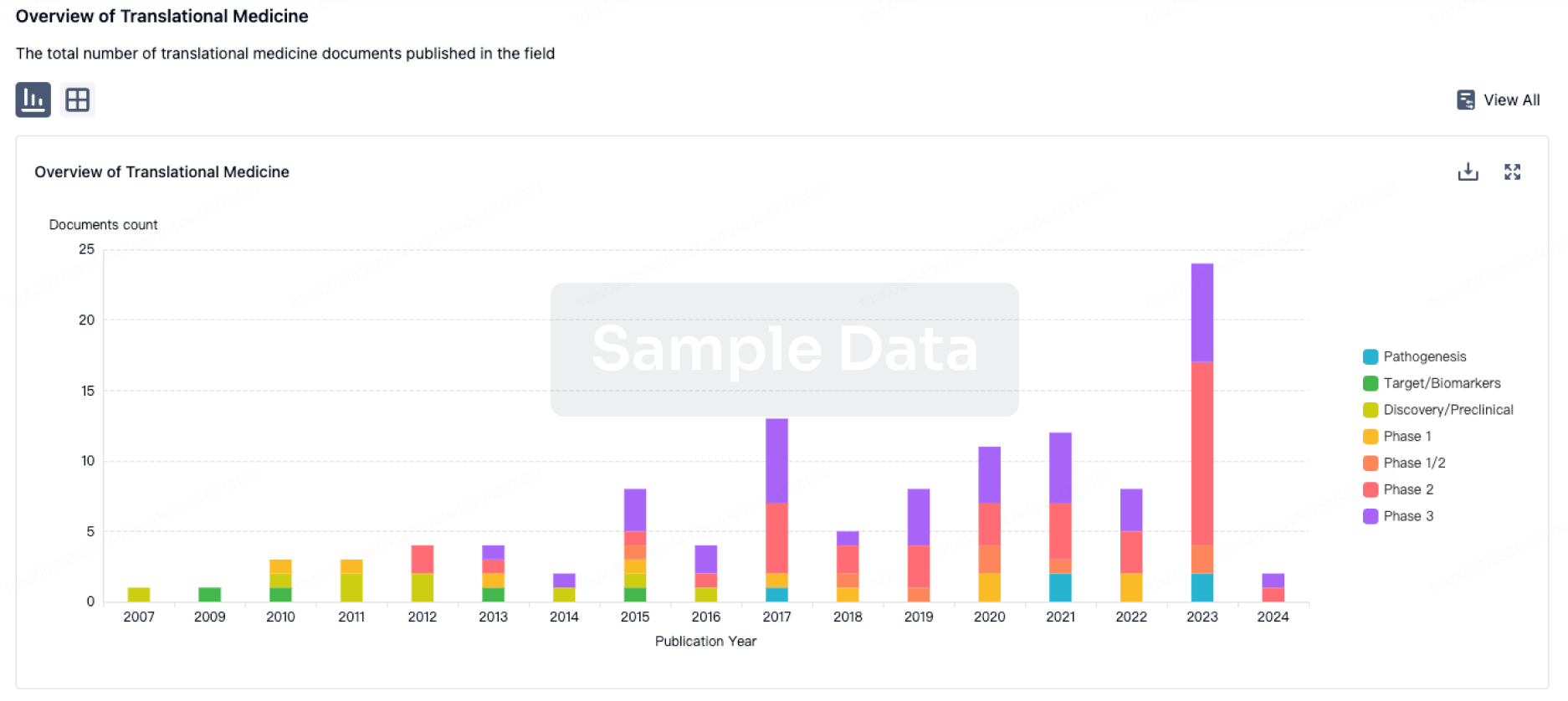
100 Translational Medicine associated with Lactobacillus plantarum TCI507
Login to view more data
100 Patents (Medical) associated with Lactobacillus plantarum TCI507
Login to view more data
4
Literatures (Medical) associated with Lactobacillus plantarum TCI50701 Aug 2018Bulletin of Entomological ResearchQ3 · AGRICULTURAL & FORESTRY SCIENCE
Microbial composition affects the performance of an artificial Tephritid larval diet
Q3 · AGRICULTURAL & FORESTRY SCIENCE
Article
Author: Pinto, R ; Rempoulakis, P ; Birke, A ; Nestel, D ; Nemny-Lavy, E ; Sela Saldinger, S
31 Oct 2013Genome Announcements
Draft Genome Sequence of Lactobacillus plantarum Strain AY01, Isolated from the Raw Material of Fermented Goat Milk Cheese
Article
Author: Zheng, Hua-Jun ; Gong, Fu-Ming ; Li, Xiao-Ran ; Zhang, Zhong-Hua ; Luo, Yi-Yong ; Liu, Chen-Jian
Food & FunctionQ2 · MEDICINE
Investigating the growth performance, meat quality, immune function and proteomic profiles of plasmal exosomes in Lactobacillus plantarum-treated broilers with immunological stress
Q2 · MEDICINE
Article
Author: Wang, Yang ; Liu, Huawei ; Zhao, Fan ; Zhang, Kai ; Zhao, Jinshan
100 Deals associated with Lactobacillus plantarum TCI507
Login to view more data
R&D Status
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
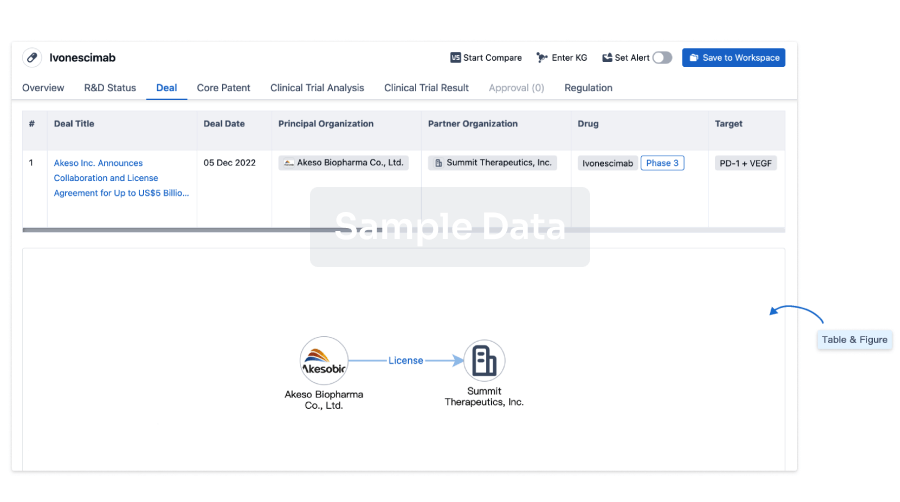
Deal
Boost your decision using our deal data.
login
or
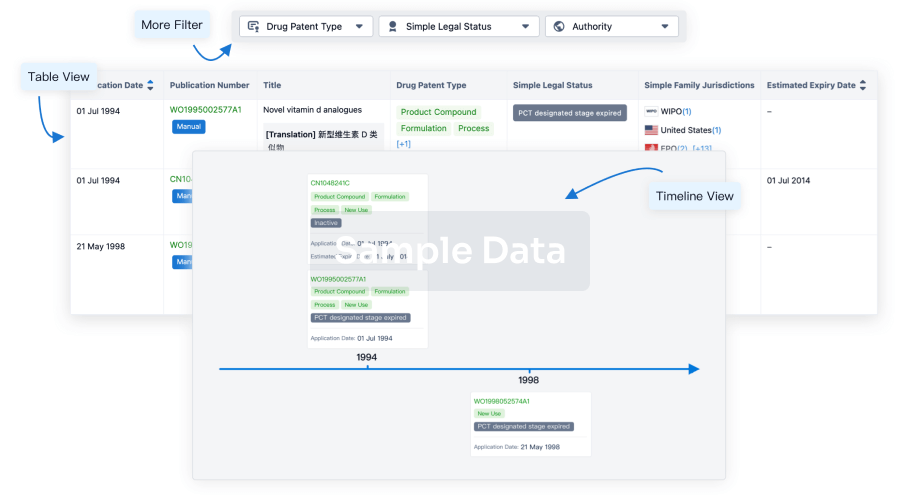
Core Patent
Boost your research with our Core Patent data.
login
or
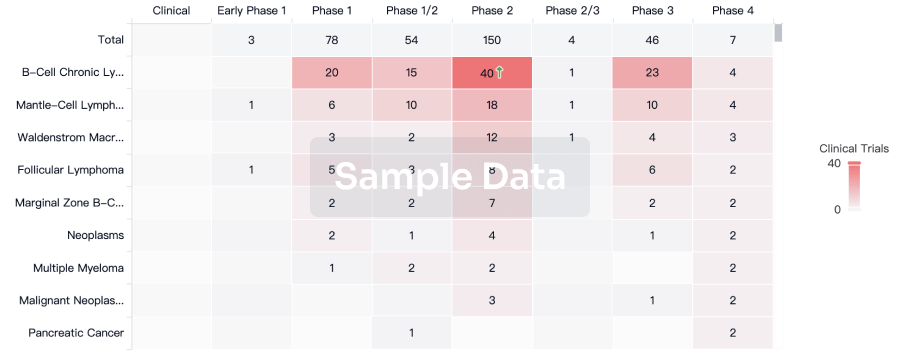
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
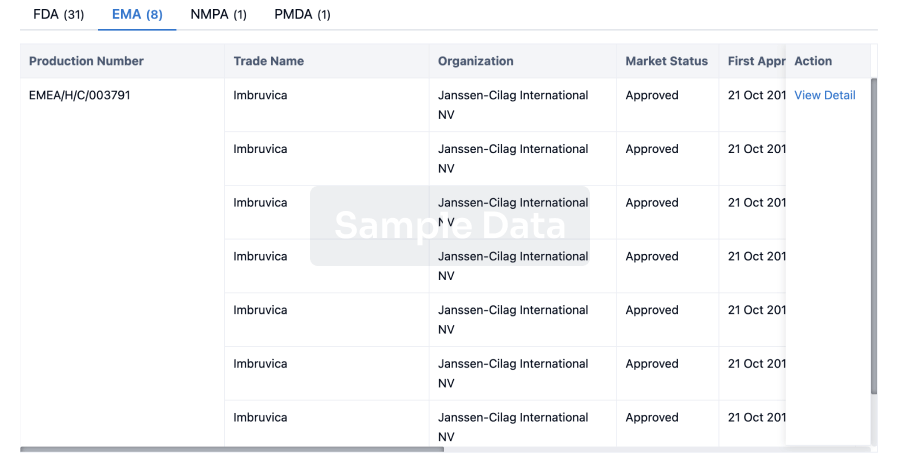
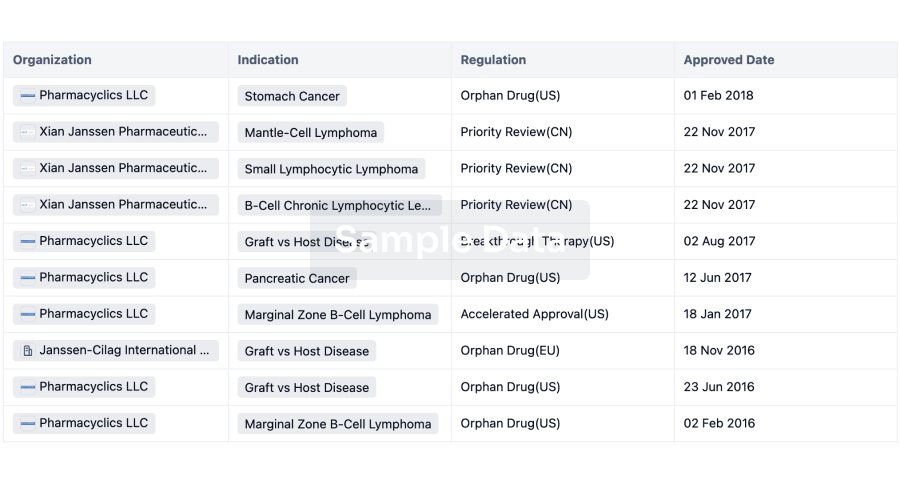
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free