Reversal of Dual Antiplatelet Therapy With Cold Stored Platelets
This study aims to determine whether cold-stored platelets (CSP) are equally, more effective, or uniquely effective at reversing the effect of dual antiplatelet therapy in healthy human subjects compared to room-temperature-stored platelets (RTP). The investigators plan to enroll healthy human subjects without risk factors for bleeding to achieve 60 complete data sets. Each subject will donate two apheresis platelet units. One platelet unit will be stored in the cold (CSP) and one platelet unit will be stored at room temperature (RTP). Subjects will be given dual anti-platelet therapy (aspirin and clopidogrel) prior to autologous transfusion of each unit. Platelet function testing will be performed before and after transfusion to measure reversal of the antiplatelet drugs.
Formula-driven vs Laboratory-guided Transfusion Practices in Bleeding Trauma Patients: A Feasibility Randomized Controlled Study
Background: Bleeding and coagulopathy still accounts for the majority of early in-hospital deaths following trauma. There have been lately several published studies suggesting that higher transfusion ratios of fresh frozen plasma (FFP), platelets (PTL) and cryoprecipitate (CRYO) to red blood cell (RBC) are associated with survival advantages. However, the evidence comes from retrospective data limited by a significant number of unaddressed confounders. In addition, the use of blood products bears known and important risks of complications.
Hypothesis: The adoption of a formula-driven transfusion practice with pre-defined ratios of FFP to PTL to RBC transfusion (1:1:1) is feasible and superior to current laboratory-guided transfusion practice in treating and/or preventing early coagulopathy improving survival rates in massively bleeding trauma patients .
Objective: To exam the feasibility of implementing a pre-defined ratio of FFP to PTL to RBC (1:1:1) transfusion protocol and its impact on a population of bleeding trauma patients.
Design: A two-year pilot feasibility randomized control trial at Sunnybrook Health Sciences Centre. Randomization: 70 patients are expected to be randomized to lab-driven or to formula-driven massive transfusion protocol and followed-up to 28 days or hospital discharge.
Study outcomes: protocol violation; in-hospital mortality by exsanguination; death at 28 days; coagulation competence defined by current standard coagulation tests (INR & PTT < 1.5 times normal; PTL ≥ 50 and Fibrinogen ≥ 1.0) or clotting factor levels ≥ 30%; correlation of current standard coagulation tests with clotting factors levels; cessation of bleeding; incidence of ALI, sepsis, MOF, transfusion-related circulatory overload, transfusion reactions; Ventilator-free days; ICU & Hospital LOS; thromboembolic events.
Intervention protocol: Transfusion of pre-defined ratios of FFP and PTL to RBC (1:1:1) (formula-driven) for the first 12h of hospitalization without coagulation tests guidance while patient is hemorrhaging or before if bleeding stops.
Statistical analysis: protocol compliance rate and in-hospital mortality rates within 24h and at 28 days will be assessed using Chi-square test. ROC analysis will be used to analyze coagulation competence.
Main expected outcomes: implementation of a formula-driven transfusion protocol is feasible and coagulation competence will be achieved faster and more efficiently in the study group.
100 Clinical Results associated with National Blood Foundation
0 Patents (Medical) associated with National Blood Foundation
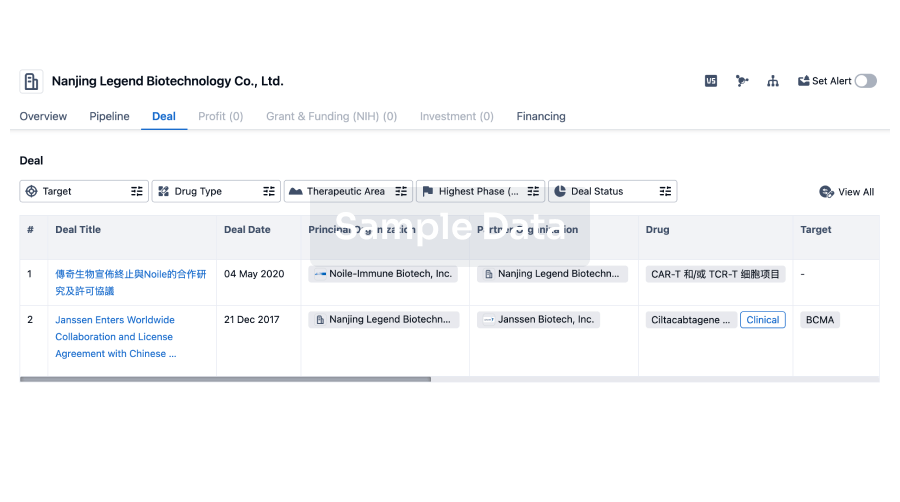
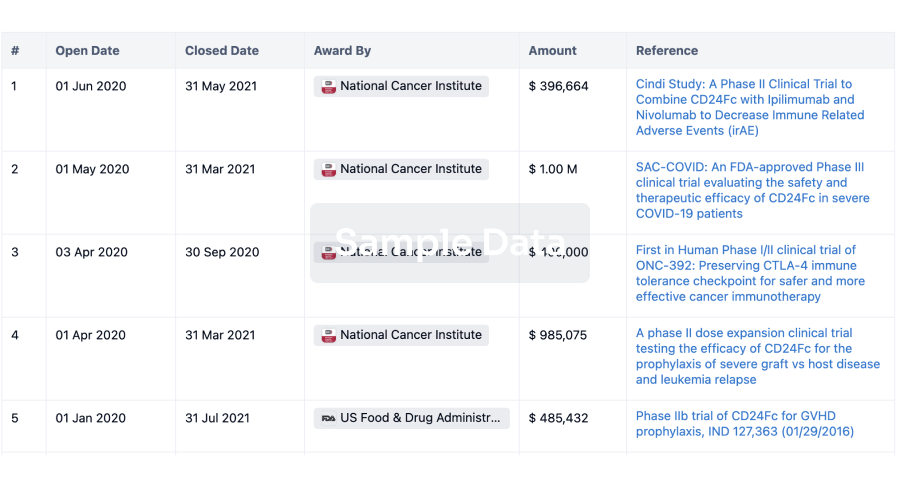
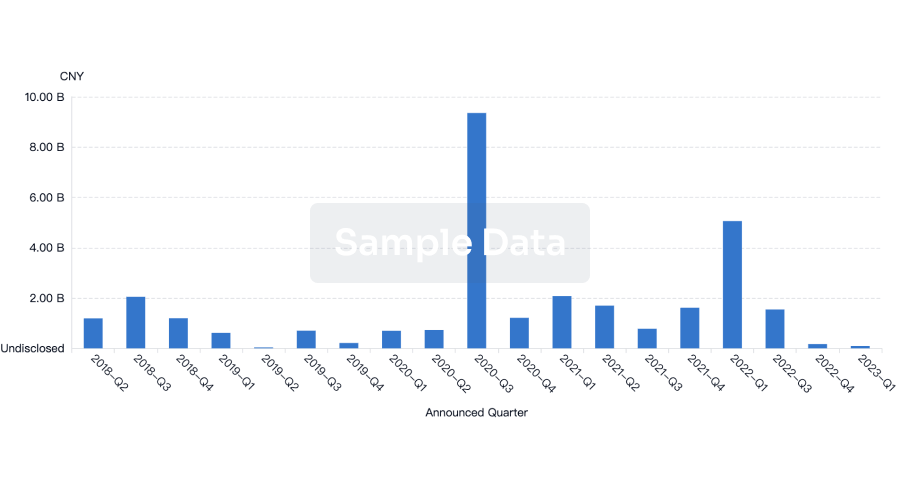
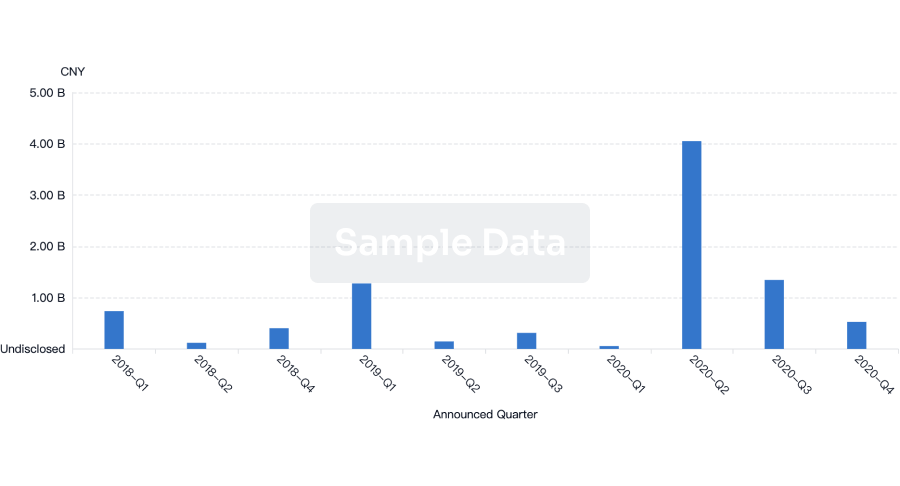
100 Deals associated with National Blood Foundation
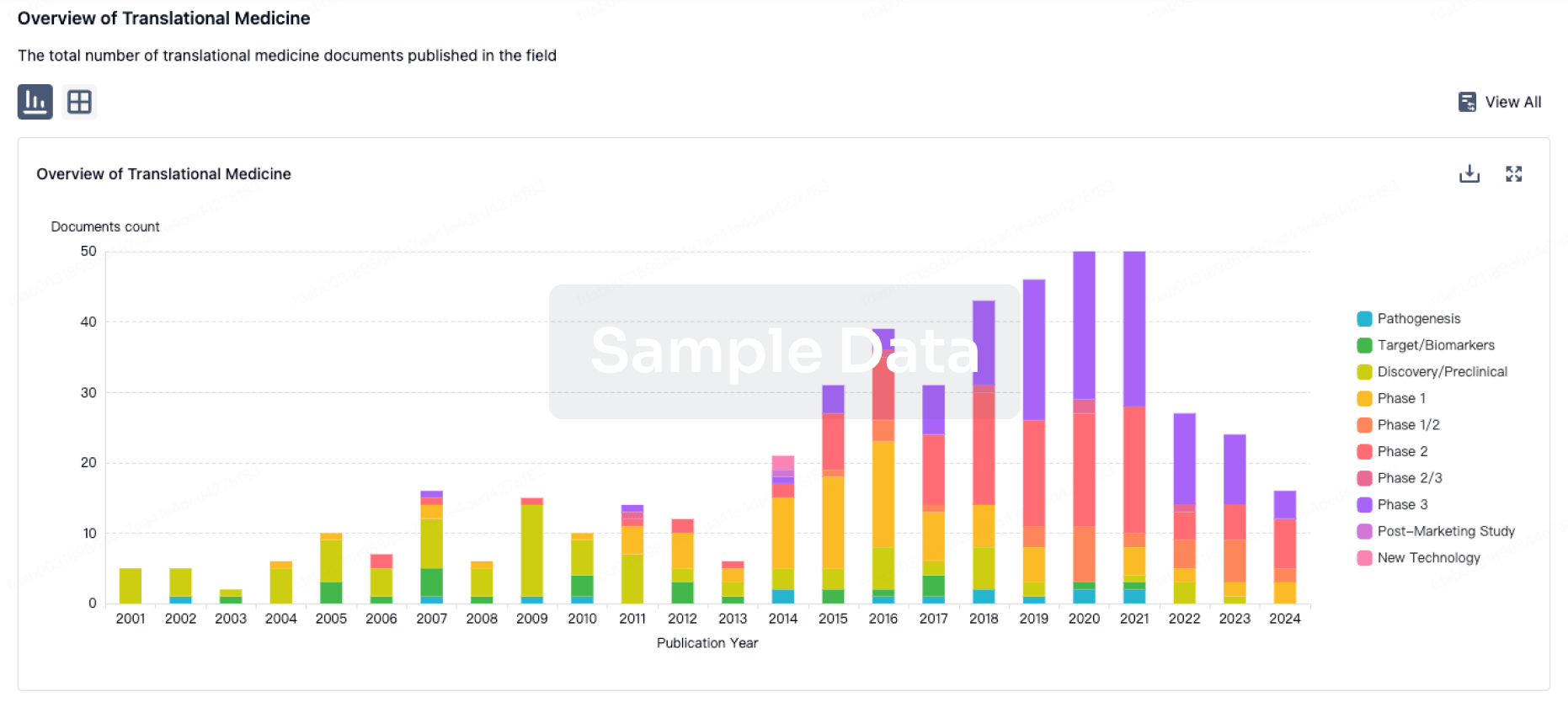
100 Translational Medicine associated with National Blood Foundation