Request Demo
Last update 08 May 2025
Bayonne Medical Center, Inc.
Subsidiary Company|1988|New Jersey, United States
Subsidiary Company|1988|New Jersey, United States
Last update 08 May 2025
Overview
Related
100 Clinical Results associated with Bayonne Medical Center, Inc.
Login to view more data
0 Patents (Medical) associated with Bayonne Medical Center, Inc.
Login to view more data
36
Literatures (Medical) associated with Bayonne Medical Center, Inc.10 Mar 2025·Cureus
A Rare Case of Idiopathic Noncirrhotic Portal Hypertension in a Young Patient
Article
Author: Aziz, Ahmed Ali ; Ali, Ijlal Akbar ; Aziz, Muhammad Ali ; Shah, Rehan ; Amir, Muhammad
13 Feb 2025·Cureus
Outcomes of Acute Pancreatitis in Patients With and Without Liver Cirrhosis: A Retrospective Analysis
Article
Author: Ali, Ijlal Akbar ; Aziz, Muhammad Ali ; Aziz, Ahmed Ali ; Shah, Rehan ; Amir, Muhammad
01 Nov 2024·Digestive Diseases and Sciences
Need for a More Objective, Inclusive, and Equitable Selection Process for Gastroenterology Fellowships
Review
Author: Gumaste, Vivek V
2
News (Medical) associated with Bayonne Medical Center, Inc.12 Jan 2024
Hudson Health System Will Operate Four Acute Care Hospitals
JERSEY CITY, N.J., Jan. 12, 2024 /PRNewswire/ -- Executive leadership at both Hudson Regional Hospital and CarePoint Health System are announcing the creation of
Hudson Health System, a new management company that will incorporate the acute care facilities of Hudson Regional Hospital and CarePoint Health.
The principals of the new network signed a letter of intent on Thursday that is the precursor to a new organizational structure and operating plan which will require approval from the New Jersey State Department of Health. Hudson Health System will be a four-hospital network including Hudson Regional Hospital, Bayonne Medical Center, Hoboken University Medical Center, and Christ Hospital in Jersey City.
"Since entering this marketplace in 2018 our team has driven a patient-focused mission that incorporates technology and engages leading healthcare professionals to deliver care under a new model,"
said Yan Moshe, Chairman of Hudson Regional who will be Chairman of Hudson Health System. "I am excited to bring our proven track record and experienced team in partnership with Dr. Moulick to build a high quality, stable health care system that the county deserves. We are all committed to bringing top quality care, physicians and efficient operations that will allow us to achieve those goals. We are grateful to Mayor Fulop and other Hudson County elected officials for their critical role in envisioning a new network that would allow these facilities and healthcare professionals to reach their potential."
The new system will continue both Hudson Regional Hospital's and CarePoint Health's demonstrated commitment to providing high-quality, affordable healthcare for local residents. The system will include both nonprofit and for-profit hospitals in an innovative new model, and it will continue to be in-network with all major insurance carriers.
"Hudson County is the most diverse and dynamic community in New Jersey, and its residents deserve nothing less than exceptional care, affordable access, the most advanced specialties and technology, and the highest caliber physicians to serve patients' needs, especially the underserved communities that rely on our facilities,"
said CarePoint President and CEO Dr. Achintya Moulick, who will be President and CEO of Hudson Health System. "Yan Moshe has shown the type of innovative leadership that will allow us to thrive in an ever-changing healthcare environment, and with adequate state support I believe we can build a hospital system that will deliver on its core mission."
"This new system expands our mutual impact far beyond and far sooner than what we could ever have achieved separately,"
says Dr. Nizar Kifaieh, CEO of Hudson Regional Hospital. "The possibilities are enormous and will energize the entire medical community to deliver that much more to the patients."
"This partnership will strengthen CarePoint's financial position and benefit our entire hospital network, from Christ Hospital and Hoboken University Medical Center which will continue to operate as non-profit safety net hospitals to Bayonne Medical Center which will still provide exceptional service to the community,"
said Dr. John Rimmer, CarePoint Chief Medical Officer. "This is an exciting moment for health care in Hudson County that will mean improved care and better patient outcomes."
Additional details about Hudson Health System will be announced in the coming days.
SUPPORT FOR HUDSON HEALTH SYSTEM FROM HUDSON COUNTY ELECTED OFFICIALS:
Jersey City Mayor Steven Fulop:
"It became clear over the last several months that Hudson County had an opportunity to create a dynamic new healthcare model. There is no greater priority than the health of our residents, and we convened the operators of our major hospitals together to create a platform that would assure quality care and enduring stability. I am pleased to say that the discussions on all sides were driven by a shared commitment to the interests of the patients. It is a complex undertaking to blend facilities and cultures and managements, but out of this effort we have arrived at an admirable place: Hudson County is now a leader in community-focused care."
State Senator Angela McKnight (D-31):
"As a safety net hospital that provides care to tens of thousands of uninsured, underserved, undocumented, unhoused, or lower income patients every year, ensuring that Christ Hospital and the rest of the CarePoint system can continue to operate is one of my highest legislative priorities. I'm ecstatic to see this partnership come to fruition and I believe that it represents a new beginning for our communities, especially for our seniors and the people who most need high-quality healthcare."
State Senator Joseph Lagana (D-38):
"This is not purely a Hudson County moment," says Senator Joseph Lagana from Paramus. "The entire state benefits when any area of the state has its healthcare improved in such a dramatic fashion. We look forward to the echoes from the advancements and innovations, that surely will result from this new network."
Hudson County Executive Craig Guy:
"Improving the quality of our health care options and delivering better patient outcomes in Hudson County is critically important, and I'm committed to working with our team, my fellow elected officials and state leaders to ensure that my constituents' needs are best served."
State Senator Raj Mukherji (D-32):
"Healthcare is a fundamental human right, but it isn't treated that way in our system of care. This oversight is particularly evident in CarePoint's treatment of a vast number of indigent patients without compensation, including our immigrant neighbors who lack documentation – denying these safety net hospitals critical support they would need to survive independently.
Ellis Island, a beacon of welcome, lies within New Jersey's waters, not New York's. Yet, New York extends emergency Medicaid to eligible undocumented immigrants and offers full Medicaid to those 65+ along with options for mixed status families. I call on my colleagues to enact a true public option for healthcare in New Jersey, broaden Medicaid eligibility beyond the current federal poverty level income percentage as CMS rules allow, and stop the cruel denial of this human right to our undocumented neighbors.
In the interim, this partnership will enable these hospitals not only to survive but thrive. I am eager to see the implementation of promised community governance at the two hospitals that will continue as nonprofits, and I want to thank the visionary leaders of both CarePoint Health and Hudson Regional Hospital for uniting in common purpose and fulfilling the critical acute care needs of Hudson County residents, needs that are both urgent and deserving."
Secaucus Mayor Michael Gonnelli:
"As the home of Hudson Regional Hospital, we have seen the incredible improvements that insightful healthcare management can bring to a community. Now, with additional resources and a plan that will service the entire county, I look forward to even greater accomplishments and expanded services to our residents."
Bayonne Mayor Jimmy Davis:
"My focus has always been on ensuring that the people of Bayonne will continue to have a full-service acute care hospital here in our city, and this agreement means that Bayonne Medical Center will not just continue providing the care our residents need but will now be able to provide enhanced services to our community. I commend everyone involved in this landmark partnership for their tireless efforts and for ensuring that all of Hudson County's residents have access to the medical care and services they deserve. Yan Moshe, the entire Hudson Regional Hospital executive team, CarePoint's executive team and all those who helped negotiate this agreement have served the residents of Bayonne and Hudson County well."
Hoboken Mayor Ravi Bhalla:
"Hoboken's primary objective has always been to ensure there is a high-functioning hospital with quality and affordable health services available for our residents. I'm pleased that this innovative new agreement aims to ensure that occurs to the greatest extent possible, and I look forward to staying in touch with all stakeholders to work through the details."
SOURCE Hudson Health System
AHA
14 Sep 2022
A “years-long systemic effort” to “destroy competition.”
Allegations of a conspiracy with real estate investors to push a health system in New Jersey into bankruptcy. Accusations of neglecting the poor and uninsured.
All of the above have made their way into a lawsuit that pits a three-hospital New Jersey health system against the largest health system in the state, accusing it of conspiracy to eliminate competition.
CarePoint Health filed the lawsuit against RWJBarnabas Health on Sept. 6. The plaintiff alleged that RWJBarnabas pursued a multi-year anti-competitive scheme to “monopolize the provision of general acute care hospital services and related health care services in northern New Jersey.”
CarePoint comprises 349-bed Christ Hospital, 224-bed Bayonne Medical Center and 348-bed Hoboken University Medical Center. RWJBarnabas Health includes 12 acute care hospitals and four children’s hospitals, along with other locations and services, including outpatient centers, ambulatory care centers, home care and hospice programs and accountable care organizations.
The lawsuit alleges RWJBarnabas conspired with real estate investors, government officials and Horizon Blue Cross Blue Shield (New Jersey’s largest payer) to usurp CarePoint’s patient revenue and push the health system into bankruptcy.
CarePoint claimed that it was RWJBarnabas’ goal to force shutdowns for Christ Hospital and Bayonne Medical Center but acquire Hoboken University Medical Center because of its more lucrative payer mix. This alleged plan “disregarded the needs of the poor, underinsured and charity care patients which CarePoint serves in its role as the safety net hospital system in Jersey City and surrounding areas,” the lawsuit stated.
The complaint said that RWJBarnabas issued a fake letter of intent to acquire Christ Hospital and Hoboken University Medical Center in 2019. Carepoint claimed that RWJBarnabas did not actually want to buy these hospitals — instead RWJBarnabas was conspiring with “real estate players” to gather market knowledge and competitive intelligence to “freeze programmatic growth and any significant hiring or construction at Christ Hospital.”
At first, CarePoint believed the offer was brought in good faith. Negotiations stopped after CarePoint began to believe RWJBarnabas had plans to hold the real estate “hostage.” RWJBarnabas circulated rumors about consolidating and closing Christ Hospital or reducing it to a small emergency department, which led to the attrition of physicians, employees and patients at the hospital, the lawsuit alleged.
The lawsuit drew attention to a satellite emergency department RWJBarnabas opened in “in coordination with Horizon” in 2017, just five blocks away from CarePoint’s Bayonne Medical Center. The resulting divergence of urgent care patients caused CarePoint to lose at least $80 million over the last three years, according to the lawsuit. Carepoint alleged that the satellite emergency department was constructed and began operating without the required approval of the New Jersey Department of Health.
Carepoint also claimed it has lost at least $227 million as a result of RWJBarnabas’ efforts to divert and steer to its Jersey City Medical Center. RWJBarnabas has been diverting EMS patient transports away from CarePoint facilities and to the medical center, particularly patients with private medical insurance or the financial means to pay for the transport and any resulting emergency or in-patient services, the lawsuit alleged. It also alleged that RWJBarnabas steered uninsured patients and those covered by Medicare or Medicaid to CarePoint facilities.
These practices represent a “flagrant disregard” of a 2016 agreement settling earlier litigation regarding ambulance service in Jersey City and the surrounding area, CarePoint said. The insurance information RWJBarnabas uses to divert and steer EMS transport was obtained through Horizon, according to the complaint.
The lawsuit also alleged that RWJBarnabas and its conspirators assert “undue influence on the NJDOH and the governor’s office to hinder CarePoint from growing programs for the community, from receiving funds for serving the underinsured and underserved and also to create roadblocks in CarePoint’s evolution into a regional powerhouse in healthcare with a stable financial base.”
RWJBarnabas’ wrongdoings violate the Sherman Antitrust Act and the New Jersey Antitrust Act, the lawsuit claimed.
A RWJBarnabas statement forcefully dismissed the allegations.
The lawsuit is “yet another in a series of baseless complaints filed by CarePoint, an organization whose leadership apparently prefers to assign blame to others rather than accept responsibility for the unsatisfactory results of their own poor business decisions and actions over the years,” a RWJBarnabas spokesperson said. The spokesperson would not comment on the specific allegations beyond what the health system said in a statement last week.
This is not the first time RWJBarnabas’ alleged anti-competitive business practices have made headlines this year. In June, the health system called off a merger with Saint Peter’s Healthcare System after the Federal Trade Commission blocked the deal, saying it would hurt competition and increase prices.
Acquisition
100 Deals associated with Bayonne Medical Center, Inc.
Login to view more data
100 Translational Medicine associated with Bayonne Medical Center, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 17 Jul 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
Translational Medicine
Boost your research with our translational medicine data.
login
or
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
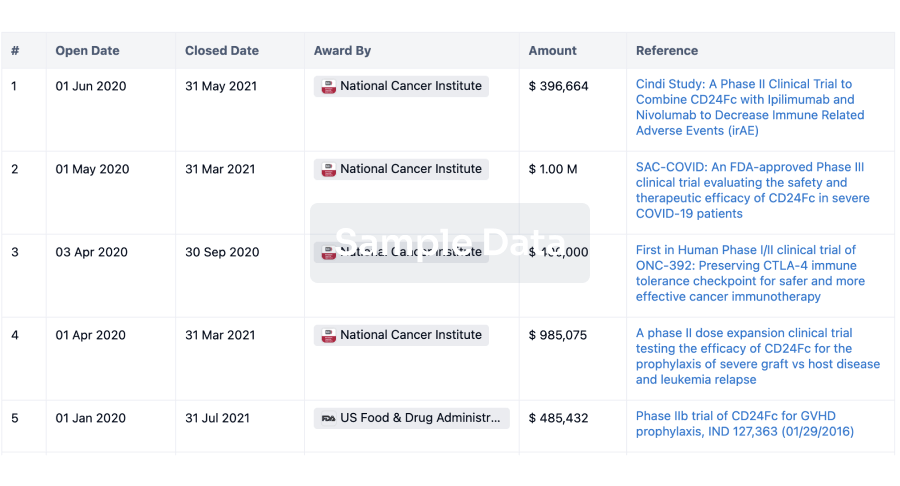
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
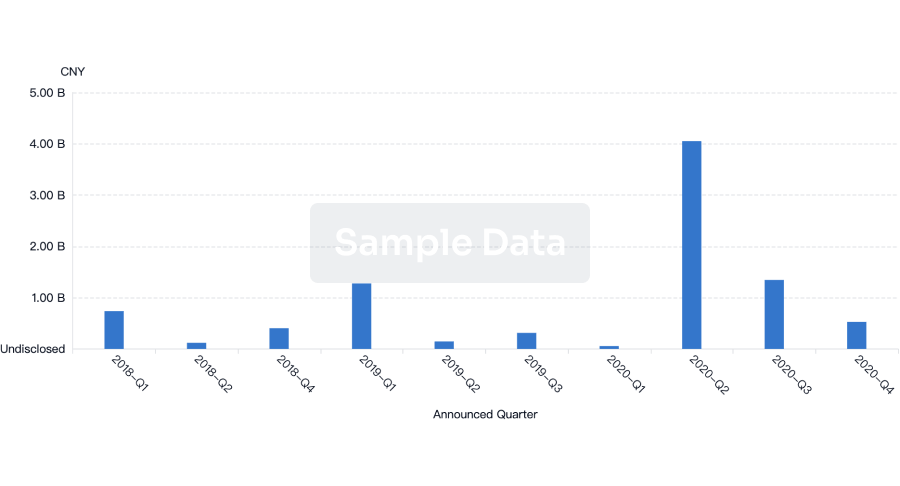
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free