Request Demo
Last update 24 Mar 2025
131 I-L19-small immunoprotein(Philogen SpA)
Last update 24 Mar 2025
Overview
Basic Info
Drug Type Radiolabeled antibody, Therapeutic radiopharmaceuticals |
Synonyms 131 I-L19-small immunoprotein, 131I-L19-SIP, I-131-L19-SIP + [5] |
Target |
Action inhibitors |
Mechanism EDB-FN inhibitors(Human fibronectin extra domain B inhibitors) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization- |
Drug Highest PhasePhase 2 |
First Approval Date- |
Regulation- |

Login to view timeline
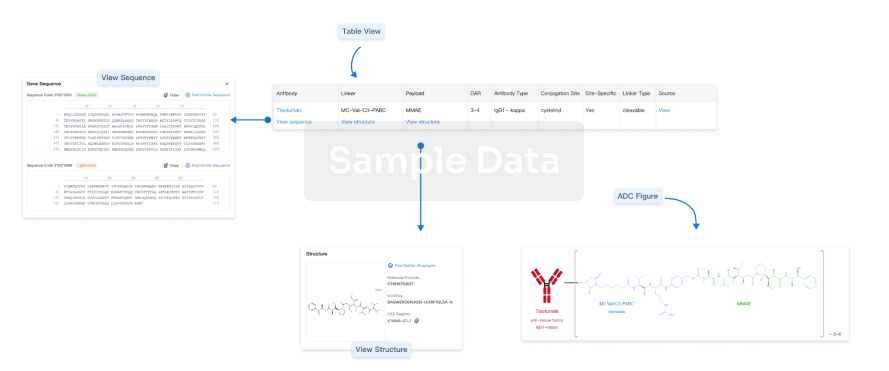
Structure/Sequence
Boost your research with our ADC technology data.
login
or
Related
3
Clinical Trials associated with 131 I-L19-small immunoprotein(Philogen SpA)NCT01124812
A Prospective Non-randomized Study of 131I-L19SIP Radioimmunotherapy (RIT) in Combination With External Beam Radiotherapy (EBRT) and Concurrent Chemotherapy in Patients With Inoperable, Locally-advanced (Stage III) NSCLC
NCT01242943
A PHASE I/II DOSE FINDING AND EFFICACY STUDY OF THE TUMOUR TARGETING HUMAN 131I-L19SIP MONOCLONAL ANTIBODY IN PATIENTS WITH CANCER
EUCTR2007-007241-12-GB
A PHASE I/II DOSE FINDING AND EFFICACY STUDY OF THE TUMOUR TARGETING HUMAN 131I-L19SIP MONOCLONAL ANTIBODY IN PATIENTS WITH CANCER - Radioimmunotherapy with 131I-L19SIP in patients with cancer
100 Clinical Results associated with 131 I-L19-small immunoprotein(Philogen SpA)
Login to view more data
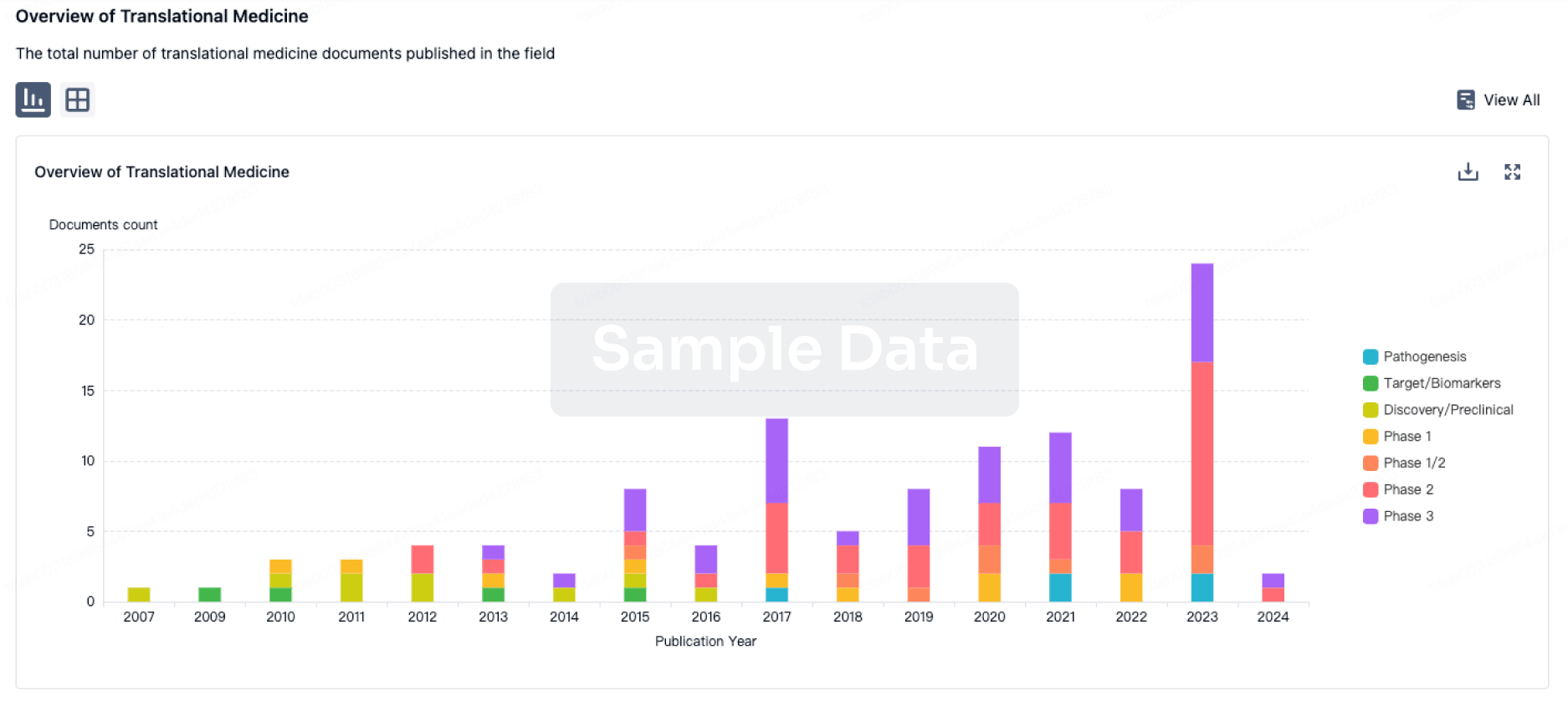
100 Translational Medicine associated with 131 I-L19-small immunoprotein(Philogen SpA)
Login to view more data
100 Patents (Medical) associated with 131 I-L19-small immunoprotein(Philogen SpA)
Login to view more data
11
Literatures (Medical) associated with 131 I-L19-small immunoprotein(Philogen SpA)01 Mar 2016Bone marrow transplantationQ3 · MEDICINE
Nivolumab in a patient with refractory Hodgkin’s lymphoma after allogeneic stem cell transplantation
Q3 · MEDICINE
Letter
Author: Schulze, A B ; Berdel, W E ; Schliemann, C ; Angenendt, L ; Stegger, L ; Lenz, G ; Weckesser, M ; Rebber, E ; Groth, C ; Lutz, M ; Schäfers, M ; Kessler, T ; Stelljes, M
Allogeneic stem cell transplantation (alloSCT) is still one of the most powerful tools for the treatment of hematol. malignancies.1 The immune-mediated graft-vs.-tumor (GVT) effect endows it with the potential to cure malignancies refractory to all other treatments.Nevertheless, it is associated with the risk of donor cell-mediated graft-vs.-host disease (GVHD), which mainly contributes to its relevant morbidity and lethality.In theory, the GVT effect might be enhanced by immune checkpoint inhibitors such as ipilimumab (anti-cytotoxic T-lymphocyte-associated protein 4), nivolumab (anti-programmed cell death 1, PD1) or pembrolizumab (anti-PD1), by releasing the brakes on GVT conveying tumor-suppressed lymphocytes.2 Nevertheless, severe graft-vs.-host (GVH) reactions might be unleashed as well.While preliminary data demonstrated no significantly increased GVHD in patients treated with ipilimumab post alloSCT,3 there is still substantial concern regarding the safety of PD1 inhibitors in this setting.In fact, increased GVHD-related lethality has been demonstrated in a murine model of acute GVHD when blocking PD-L1.4 Recently, a report on a patient receiving pembrolizumab for malignant melanoma about 20 years after alloSCT reported no development of GVHD.5 However, there were no data on donor chimerism reported and lack of donor immune cells might be a reasonable cause for lack of GVHD development.Hodgkin's lymphoma (HL) is a neoplastic disease of lymphoid origin, that can initially be cured in >75% of patients using chemotherapy, often followed by consolidating radiation.6 Relapsed or refractory (r/r) patients might be salvaged by high-dose therapy and autologous stem cell transplantation.After high-dose therapy, the antibody-drug conjugate brentuximab vedotin (BV) demonstrated very promising results both as consolidation and salvage treatment and is approved in this setting.7, 8 In highly refractory cases alloSCT is considered as a therapeutic option in eligible patients.9 Recently, checkpoint inhibition by nivolumab demonstrated a remarkable overall response rate of 87% including 17% complete remissions (CR) in 23 patients with r/r HL.10 The benefit of PD1 inhibition in this setting is furthermore supported by preliminary results of pembrolizumab in 15 r/r patients achieving similar responses.11 While the latter trial allows the inclusion of patients 5 years post alloSCT, no such patient has been reported yet.Here, we report the first patient to our knowledge successfully treated with nivolumab after alloSCT.In May 2012 an 18-yr-old man was diagnosed with classical HL involving mediastinal and hilar lymph nodes as well as the middle lobe of the lung corresponding to a stage IV B (fever).Risk factors according to the German Hodgkin Study Group classification system included an erythrocyte sedimentation rate above 30 mm/h with B symptoms, a mediastinal mass on chest X-ray measuring more than one-third of the thoracic diameter (21/31 cm) and extranodal involvement (lung).Following prephase treatment with prednisolone, the patient received six cycles BEACOPP-escalated (bleomycin, etoposide, adriamycin, cyclophopshamide, vincristine, prednisolone and procarbazine).In Oct. 2012, final examination by 18F-fluorodeoxyglucose (FDG)-positron emission tomog. (PET)/computed tomog. (CT) demonstrated a CR of the mediastinal and hilar lymph nodes, but metabolically active paramediastinal residuals in the middle lobe.Unfortunately, the disease immediately progressed even before consolidating radiotherapy could be initiated.The patient received two cycles of DHAP (dexamethasone, high-dose cytarabine and cisplatin) complemented by two cycles of Dexa-BEAM (dexamethasone, carmustine, etoposide, cytarabine and melphalan) due to insufficient response on interim staging, followed by high-dose BEAM and autologous stem cell transplantation.This achieved a partial remission with residual metabolically active lesions in the mediastinum and in the right lung that were subjected to radiotherapy with 30.6 Gy.Only 3 wk after completion of radiotherapy in August 2013, the patient was again submitted to our department with fever.Staging demonstrated multifocal progressive disease, which was histol. confirmed by mediastinoscopic lymphadenectomy.At that point, a search for a matched unrelated donor for alloSCT was initiated.As a bridge to transplant the patient received five cycles of BV, resulting in a mixed response on 18F-FDG-PET/CT with regressive nodal disease, but progressing lymphoma lesions in the lung.In Dec. 2013, following conditioning with treosulfan (3 × 14 g/m2), fludarabine (5 × 30 mg/m2) and antithymocyte globulin (2 × 20 mg/kg), the patient was transplanted from an HLA-matched unrelated donor.There was no development of acute or chronic GVHD post transplantation.However, after an initial minor response, his disease already progressed 2 mo after transplantation.Considering this short response, we decided against the use of donor lymphocyte infusions (DLI).Treatment with BV was resumed with no response after 3 cycles.In July 2014, an exptl. treatment with a single dose of the vascular-targeting radioimmunoconjugate 131I-L19-SIP (2.2 GBq) that has previously demonstrated marked responses in refractory cases of HL (reference12) led to a good response of the preexistent lesions, but multiple new lesions at previously non-involved sites developed.The patient was treated with CEVD (lomustine, etoposide, vindesine, dexamethasone) chemotherapy, again leading to a mixed response with regressive intrathoracic and retroperitoneal lesions, but new liver and bone lesions.At that time, the patient's general condition progressively deteriorated accompanied with nausea, loss of appetite, severe B symptoms and significant loss of weightHe was bedridden most of the time, corresponding to a Karnofsky performance index of only 30%.Considering the high response rates in r/r HL, recently reported by Ansell et al.,10 we decided to initiate an off-label therapy with the anti-PD1 antibody nivolumab.The patient consented and received a single dose of nivolumab at 3 mg/kg (approximated to 200 mg absolute) in June 2015.Treatment was well tolerated with mild fever during the first 2 h after application being the only side effects.Within the first week after infusion, the patient's B symptoms disappeared and his clin. condition drastically improved over the following weeks (Karnofsky performance index 90%).Most importantly, there was no clin. evidence of GVHD induction.An 18F-FDG-PET/CT performed 4 wk after infusion revealed a complete metabolic response (Figure 1) and therapy with nivolumab is currently being continued.Of note, there was an unspecific FDG uptake in some parts of the colon after nivolumab.Although this could have many causes, including enteritis or even physiol. peristalsis, an unspecific T-cell activation causing a subclin. GVH reaction in the gut cannot be excluded.13 Chimerism analyses showed a complete donor cell chimerism (100%) in peripheral blood during the whole treatment period after alloSCT.Despite the generally favorable prognosis of HL, the prognosis of primary refractory patients, including those relapsing within 3 mo after first-line treatment, is poor, with a 5-yr overall survival of only 26%.6 Nevertheless, some of them can still profit from alloSCT with reduced intensity conditioning, mainly due to a GVT or 'graft-vs.-Hodgkin's-lymphoma' effect.6, 9, 14 Patients relapsing after alloSCT might be treated with DLI and/or BV, but supporting evidence is scarce.9 Recently, some studies demonstrated enhanced expression of PD-L1 in HL due to 9p24.1 amplification, chromosomal rearrangements and Epstein-Barr virus infection.2 This conceivably results in suppression of an anticancer immune response, as supported by the impressive therapeutic potential of PD1 inhibitors in r/r HL patients.10, 11 However, while it appears particularly appealing to reverse the suppression of allogeneic GVT effects with PD1 inhibition in the situation of HL relapse after alloSCT, special caution has to be taken in the context of an allogeneic immune system given the role of the PD1 axis in the pathophysiol. of GVHD as well.4 In the presented case of a patient with HL refractory to multiple lines of therapy including alloSCT and BV, nivolumab achieved a remarkable and fast response, suggesting PD1 inhibition to be a powerful means for unleashing the GVT effect in the immunosuppressive microenvironment of HL.However, we did not perform mechanistic studies and another potential cause might be a disruption of the HL supporting infiltrating leukocytes independent of a GVT effect.Importantly, despite recent concerns, there were no signs of GVHD induction in our patient.While the mice in the study of Saha received PD1/PD-L1 inhibition from day one after transplantation,4 our patient received nivolumab 19 mo after alloSCT.Thus, GVHD might be more responsive to PD1/PD-L1 inhibition during the early phase of transplantation potentially triggering severe GVH reactions in the context of conditioning-related inflammation of host tissues.In addition, our patient had never developed signs of GVHD post transplantation and patients with a history of GVHD might be at higher risk of GVHD exacerbation by releasing the brakes on existing alloreactive cells.Furthermore, follow-up is short and it is entirely conceivable that GVHD might still occur after months of treatment, similar to immune-related adverse events of checkpoint inhibition in non-transplanted patients.15 Nevertheless, more established post-alloSCT treatments such as DLIs are also associated with the risk of GVHD exacerbation.16 Thus, it seems reasonable to investigate nivolumab in a larger group of patients in this desperate situation.However, its regular use in this setting cannot be recommended on the basis of a single experience.
01 Jan 2014Journal of Cancer Research and Clinical Oncology
Abundant in vitro expression of the oncofetal ED-B-containing fibronectin translates into selective pharmacodelivery of 131I-L19SIP in a prostate cancer patient
Article
Author: Giovannoni, Leonardo ; Menssen, Hans D. ; Locher, Ricarda ; Duerkop, Horst ; Hirsch, Burkhard ; Neri, Dario ; Bombardieri, Emilio ; Erba, Paola A.
PURPOSE:
The extradomain B of fibronectin (ED-B) is a promising vascular target for selective pharmacodelivery in cancer patients. We analyzed a large series of prostatectomies from patients with prostate cancer, hyperplastic prostate disease, and normal prostates to study extent and tumor-selectivity of ED-B expression.
METHODS:
Using immunohistology, 68 adenocarcinomas of the prostate or prostate cancer-inflicted lymph nodes, 4 samples of benign prostatic hyperplasia, and 6 normal prostate glands were studied for ED-B expressing newly formed blood vessels. Further, we treated an advanced prostate cancer patient with the anti-ED-B antibody (131)I-L19SIP to study in vivo target accessibility.
RESULTS:
ED-B-positive blood vessels were found significantly more frequent in prostate cancers as compared with peritumoral prostate tissues or normal prostate glands, independent of tumor differentiation. The ED-B-positive blood vessels' density was 97 (±23), 65 (±9), and 59 (±9)/mm(2) in G3, G2, and G1 prostate cancers, respectively, and 7 (±5)/mm(2) in normal prostate glands. In high-grade (G3) prostate cancers, also the peritumoral tissue showed a higher density of ED-B vessels than normal prostate glands. Similar results were obtained when ED-B-positive vessel density was expressed as a fraction of CD34-positive vessel density. Finally, selective uptake of ED-B-binding (131)I-L19SIP to tumor lesions was found in an advanced prostate cancer patient by whole-body planar scintigraphy.
CONCLUSIONS:
ED-B-positive blood vessels were found to a large extent in prostate cancer tissues, but only rarely in normal prostates or benign prostatic hyperplasia. Whole-body planar scintigraphy in a prostate cancer patient confirmed selective uptake of (131)I-L19SIP in the prostate cancer tissues, qualifying ED-B as a promising target for selective pharmacodelivery of anticancer agents in prostate cancer.
01 May 2011European journal of cancer (Oxford, England : 1990)Q1 · MEDICINE
Microvascular biodistribution of L19-SIP in angiogenesis targeting strategies
Q1 · MEDICINE
Article
Author: Güliz Parmaksiz ; Eveline Trachsel ; Dario Neri ; Peter Vajkoczy ; Simon H. Bayerl ; Ralf Erber ; Melina Nieminen ; Marcus Czabanka ; Hans D. Menssen
INTRODUCTION:
Various strategies using L19-mediated fibronectin targeting have become useful clinical tools in anti-tumour therapy and diagnostics. The aim of our study was to characterise the microvascular biodistribution and binding process during tumour angiogenesis and after anti-angiogenic therapy.
MATERIALS AND METHODS:
SF126 glioma and F9 teratocarcinoma cells were implanted into dorsal skin fold chambers (SF126: n = 4; F9: n = 6). Using fluorescence and confocal intravital microscopy the biodistribution process was assessed at t = 0 h, t = 4 h and t = 24 h after intravenous application of Cy3-L19-SIP. Sunitinib treatment was applied for six days and microscopy was performed 2 and 6 days after treatment initiation. Analysed parameters included: vascular and interstitial binding, preferential binding sites of L19-SIP, microvascular blood flow rate, microvascular permeability. Histological analysis included CD31 and DAPI.
RESULTS:
L19-SIP showed a specific and time-dependent neovascular binding with a secondary extravasation process reaching optimal vascular/interstitial binding ratio 4 hours after iv administration (F9: L19-SIP: vascular binding: 74.6 ± 14.5; interstitial binding: 46.8 ± 12.1; control vascular: 22,2 ± 16.6). Angiogenic sprouts were preferred binding sites (F9: L19-SIP: 188 ± 15.5; RTV: 90.6 ± 13.5). Anti-angiogenic therapy increased microvascular hemodynamics (SF126: Su: 106.6 ± 13.3 μl/sec; Untreated: 19.7 ± 9.1 μl/sec) and induced increased L19-SIP accumulation (SF 126: t24; Su: 92.6 ± 2.7; Untreated: 71.9 ± 5.9) in therapy resistant tumour vessels.
CONCLUSION:
L19-SIP shows a time and blood-flow dependent microvascular biodistribution process with angiogenic sprouts as preferential binding sites followed by secondary extravasation of the antibody. Microvascular biodistribution is enhanced in anti-angiogenic-therapy resistant tumour vessels.
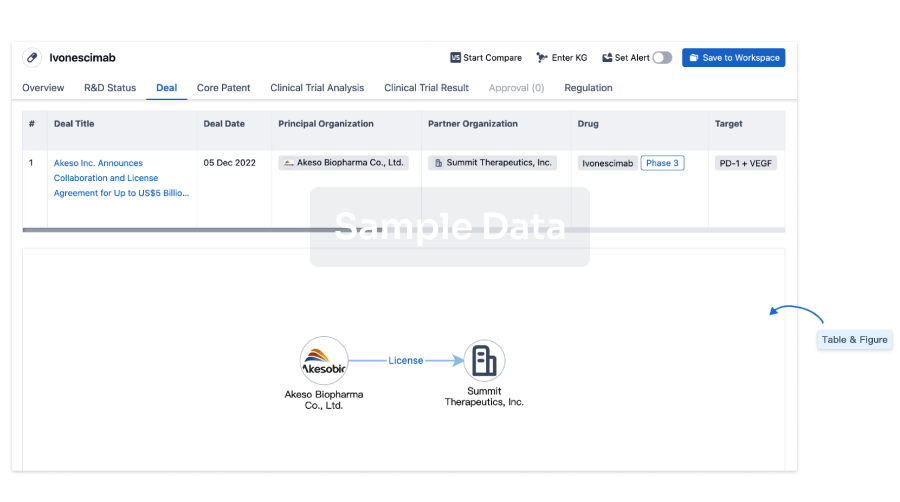
100 Deals associated with 131 I-L19-small immunoprotein(Philogen SpA)
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | 131 I-L19-small immunoprotein(Philogen SpA) | - | - |
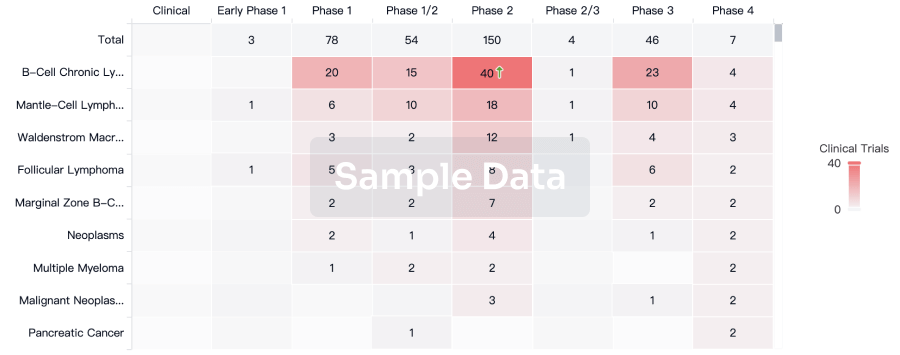
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Brain Cancer | Phase 2 | Italy | - | |
| Brain Cancer | Phase 2 | United Kingdom | - | |
| Hematologic Neoplasms | Phase 2 | - | - | |
| Hodgkin's Lymphoma | Phase 2 | - | - | |
| Solid tumor | Phase 2 | European Union | - | |
| Locally Advanced Lung Non-Small Cell Carcinoma | Phase 1 | Italy | 01 May 2010 | |
| Non-small cell lung cancer stage III | Phase 1 | Italy | 01 May 2010 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 1 | - | xqgmnouotx(tkgafzgiws) = fbtadmouxn ycizlshyqm (xqlvyvxxti ) | - | 20 May 2010 | |||
Phase 1/2 | 12 | jmyqzsrdil(kwgdciyoja) = cymopmwjwr qtrokeiumd (ggjlxgdftl ) | - | 20 May 2010 | |||
Phase 1 | 37 | xyudrgxtlu(szothclqqm) = bjrhahnzqo gcwxngzkwf (izzronouhd ) View more | - | 20 May 2008 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
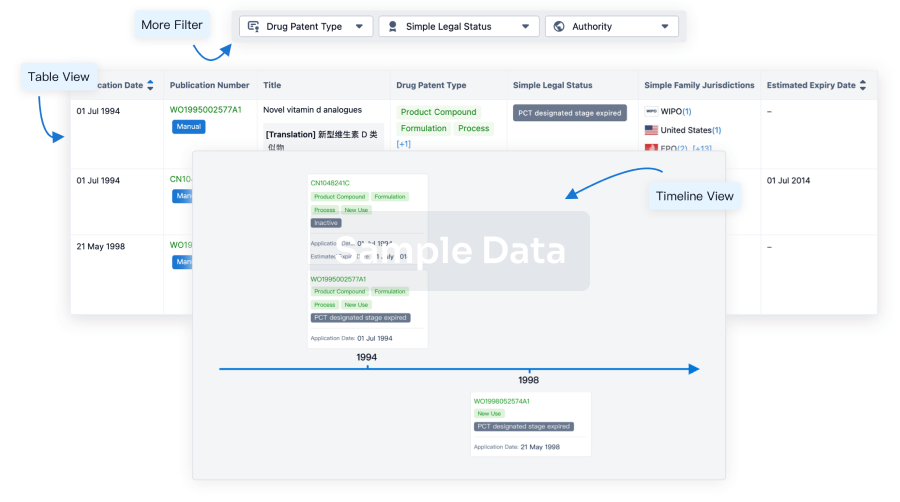
Core Patent
Boost your research with our Core Patent data.
login
or
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
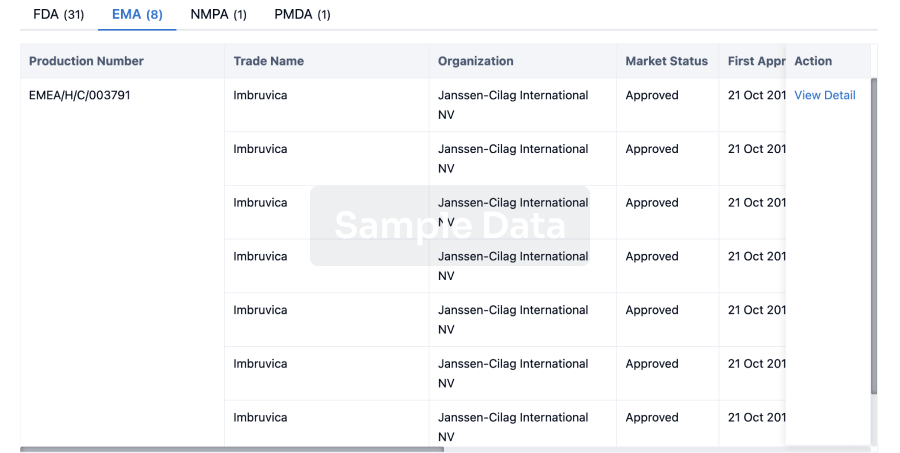
Approval
Accelerate your research with the latest regulatory approval information.
login
or
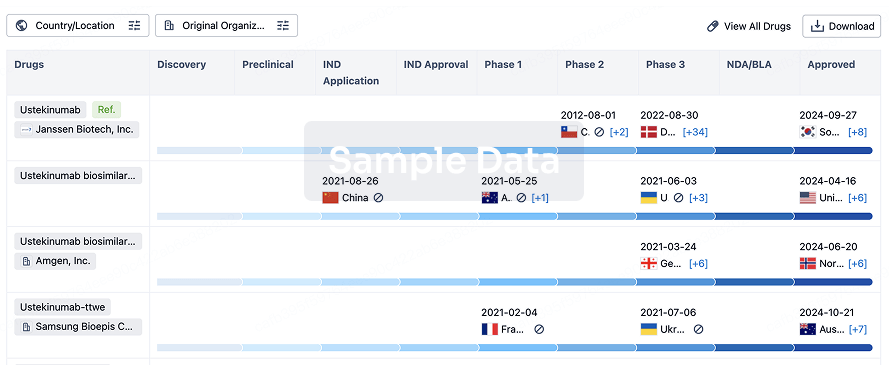
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
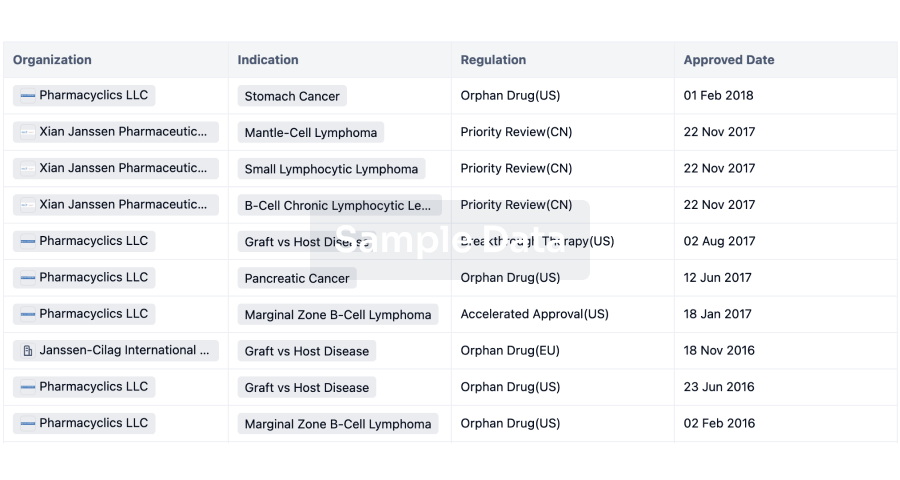
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free