Request Demo
Last update 23 Jan 2025
Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)
Last update 23 Jan 2025
Overview
Basic Info
Drug Type Prophylactic vaccine, Multivalent vaccine |
Synonyms 23-Valent Pneumococcal Polysaccharide Vaccine, 23价肺炎球菌多糖疫苗(北京民海生物科技有限公司) |
Target- |
Mechanism Immunostimulants |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Inactive Organization- |
Drug Highest PhaseApproved |
First Approval Date CN (12 Aug 2018), |
Regulation- |
Login to view timeline
Related
4
Clinical Trials associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)CTRI/2021/09/036860
A Randomized, Double-blinded, Multicenter Phase III Clinical Trial to Evaluate the Immunogenicity and Safety of 23-Valent Pneumococcal Polysaccharide Vaccine in Healthy Adults
RBR-7ymz2q
Strategies to optimize the access of adults with clinical indications to the 23-valent Pneumococcal Polysaccharide Vaccine within the Brazilian National Public Health System. - SOAP-23: Strategies to Optimize Access to 23-valent Pneumococcal polysaccharide vaccine among adults

ChiCTR2000030009
A Randomized, Blinded, Parallel Controlled, Phase III Clinical Trial for Evaluation of Immunogenicity and Safety of 23-Valent Pneumococcal Polysaccharide Vaccine in Healthy Volunteers Aged 2 Years and Above
100 Clinical Results associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)
Login to view more data
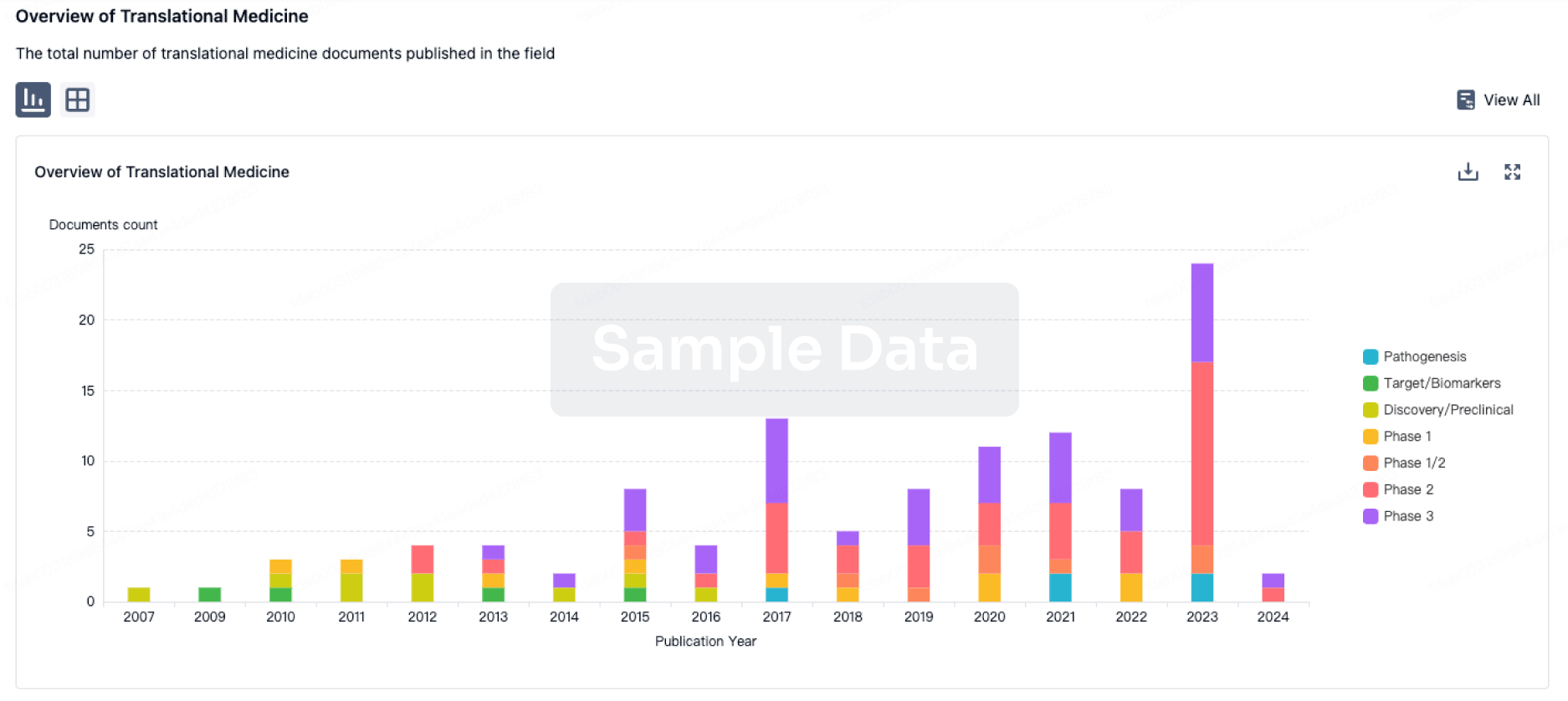
100 Translational Medicine associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)
Login to view more data
100 Patents (Medical) associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)
Login to view more data
571
Literatures (Medical) associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)12 Jan 2025Zhonghua jie he he hu xi za zhi = Zhonghua jiehe he huxi zazhi = Chinese journal of tuberculosis and respiratory diseases
[Chinese expert consensus on the diagnosis and treatment of pneumonia in the elderly (2024 Edition)].
Article
01 Jan 2025Vaccine
Safety, reactogenicity, and immunogenicity of a novel 24-valent pneumococcal vaccine candidate in healthy, pneumococcal vaccine-naïve Japanese adults: A phase 1 randomized dose-escalation trial
Article
Author: Sebastian, Shite ; Haranaka, Miwa ; Chichili, Gurunadh R ; Malley, Richard ; Oizumi, Yuki ; Borys, Dorota ; Hashimoto, Atsuki ; Nakano, Takashi ; Smulders, Ronald ; Ebara, Masaki ; Iwahana, Mioko ; Nanra, Jasdeep
01 Jan 2025Vaccine
Cost-effectiveness of 15-valent or 20-valent pneumococcal conjugate vaccine for U.S. adults aged 65 years and older and adults 19 years and older with underlying conditions
Article
Author: Leidner, Andrew J ; Kobayashi, Miwako ; Pilishvili, Tamara ; Stoecker, Charles ; Rosenthal, Melissa ; Cho, Bo-Hyun
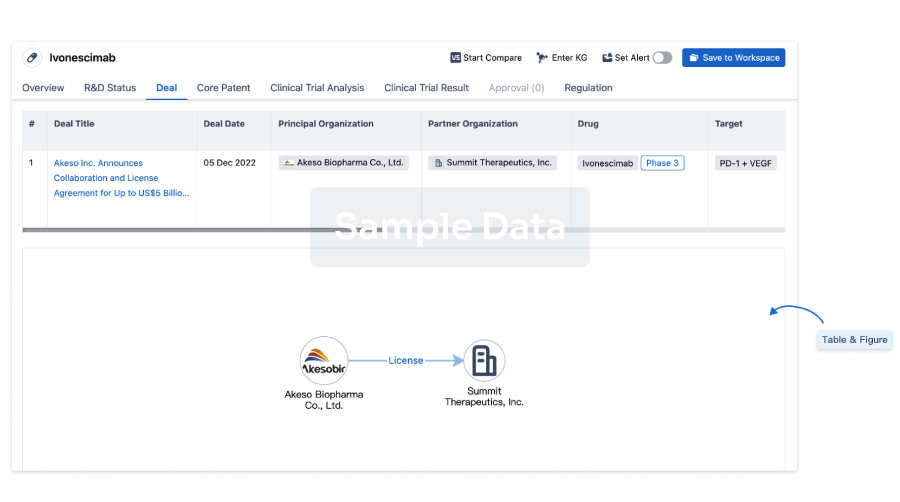
100 Deals associated with Pneumococcal polysaccharide vaccine 23-valent(Beijing Minhai Biological Technology Co., Ltd.)
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Bacteremia | CN | 12 Aug 2018 | |
| Meningitis | CN | 12 Aug 2018 | |
| Otitis Media | CN | 12 Aug 2018 | |
| Pneumonia | CN | 12 Aug 2018 |
Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Encephalitis | Phase 2 | CN | 26 Oct 2011 | |
| Pneumococcal Infections | Preclinical | CN | 30 Jan 2022 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Not Applicable | 89 | tnltwewath(ajugpbwjto) = iuevtlrydg flkcxonnzm (gnaoszntpw ) View more | - | 01 Jan 2006 | |||
tnltwewath(ajugpbwjto) = jgcnrcnrtt flkcxonnzm (gnaoszntpw ) View more |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
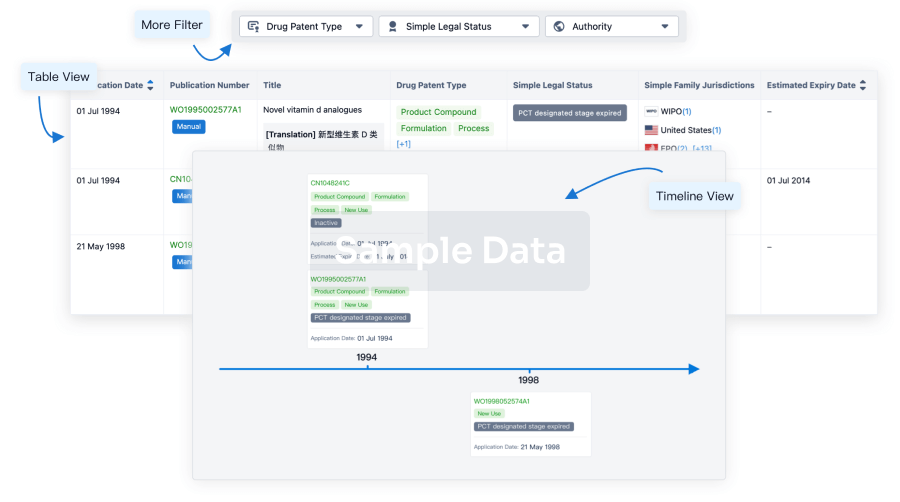
Core Patent
Boost your research with our Core Patent data.
login
or
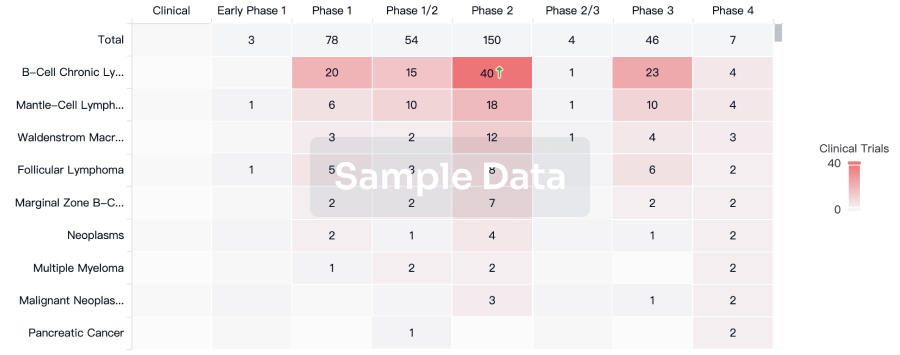
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free