Request Demo
Last update 23 Jan 2025
Swedish Match AB
Last update 23 Jan 2025
Overview
Related
ISRCTN13589495
Nicotine plasma concentrations, pharmacokinetics, and pharmacodynamics following single doses of nicotine pouches with a new format in current, daily oral tobacco/nicotine pouch users
NCT06568900
A Randomized Controlled Trial to Evaluate the Impact of ZYN Nicotine Pouch Products on Cigarette Usage and Biomarkers of Exposure in Adult Smokers Over a 12-week Period
ISRCTN38557348
Assessing biomarkers of exposure in plasma and urine in current, daily users of nicotine pouches, tobacco-based snus, or combustible cigarettes, or nonusers of tobacco/nicotine products.
100 Clinical Results associated with Swedish Match AB
Login to view more data
Login to view more data
01 Sep 2019International Journal on Interactive Design and Manufacturing (IJIDeM)
Development of virtual reality support to factory layout planning
Author: Jonatan Berglund ; Åsa Fast-Berglund ; Zhiping Wang ; Liang Gong ; Björn Johansson ; Tobias Börjesson
01 Dec 2014Medical OncologyQ4 · MEDICINE
Perforin, CD28 and CD95 expression in circulating CD4 and CD8 cells as predictors of head and neck (H&N) cancer patient survival
Q4 · MEDICINE
Article
Author: Anders Wikby ; Nongnit Laytragoon-Lewin ; Freddi Lewin ; Sture Löfgren ; Jan Lundgren ; Fredrik Jönson ; Lars Erik Rutqvist
01 Mar 2014Journal of Cancer Research and Clinical Oncology
Plasma tumor necrosis factor-α and C-reactive protein as biomarker for survival in head and neck squamous cell carcinoma
Article
Author: Freddi Lewin ; Sture Löfgren ; Lars-Erik Rutqvist ; Nongnit Laytragoon-Lewin ; Jan Lundgren ; Bengt-Åke Andersson ; Mats Nilsson
100 Deals associated with Swedish Match AB
Login to view more data
100 Translational Medicine associated with Swedish Match AB
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 24 Feb 2025
No data posted
Login to keep update
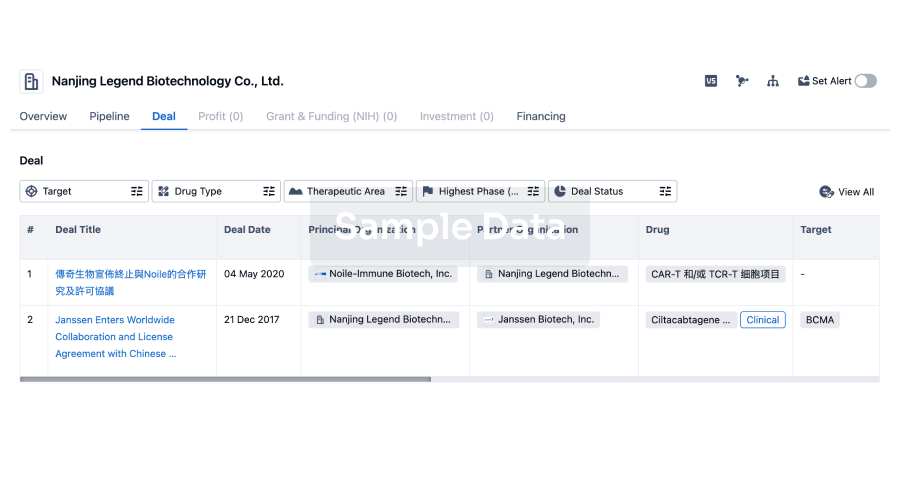
Deal
Boost your decision using our deal data.
login
or
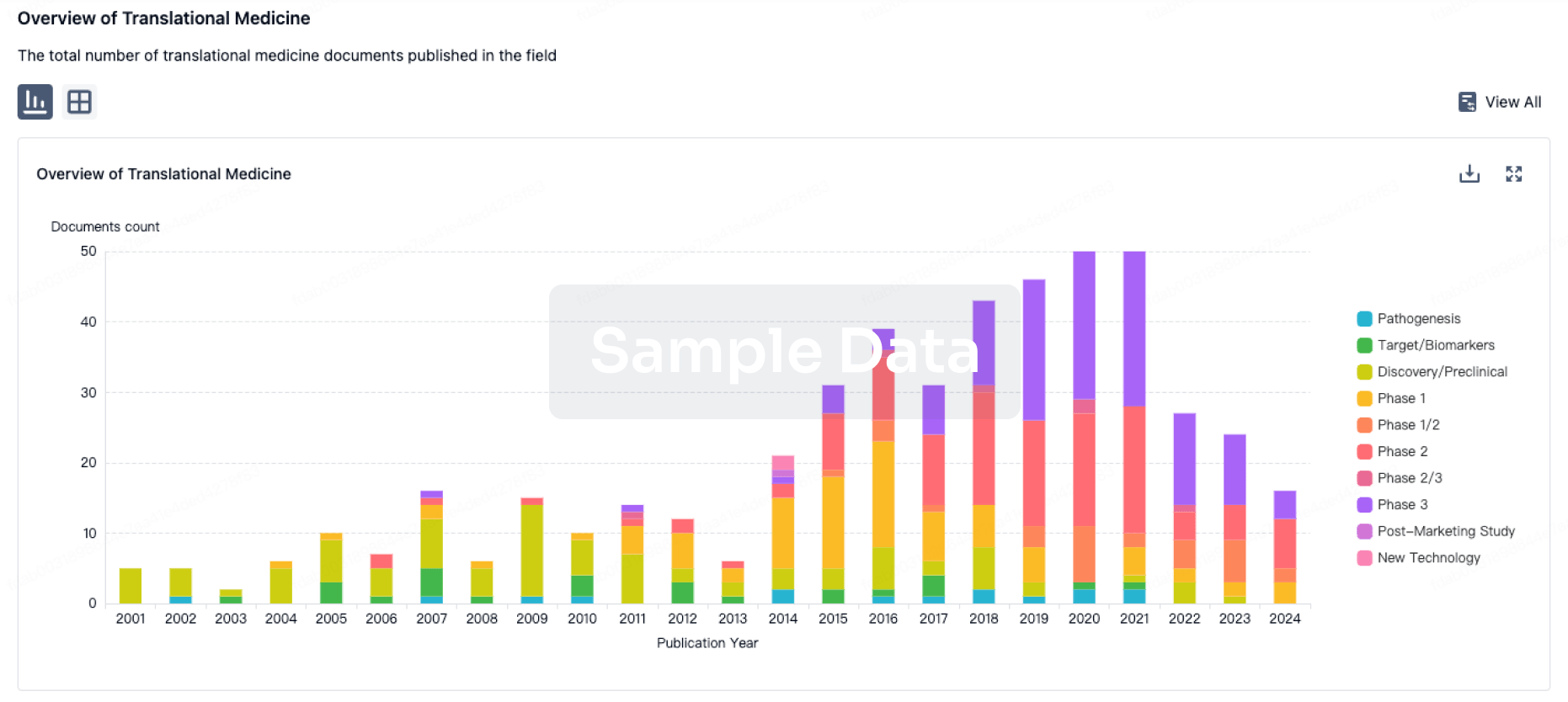
Translational Medicine
Boost your research with our translational medicine data.
login
or
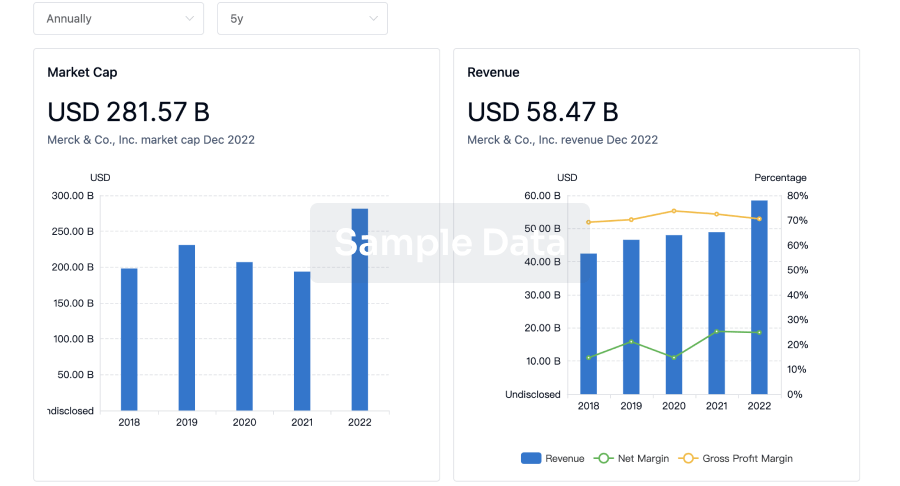
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
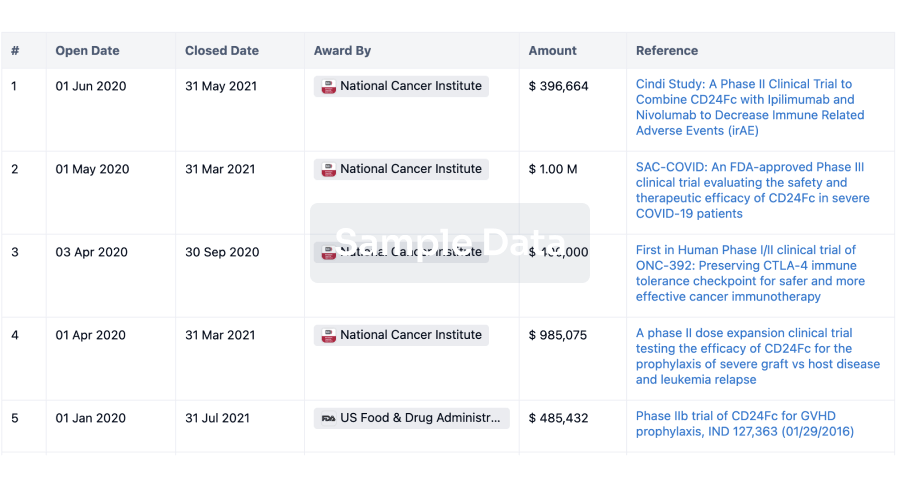
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
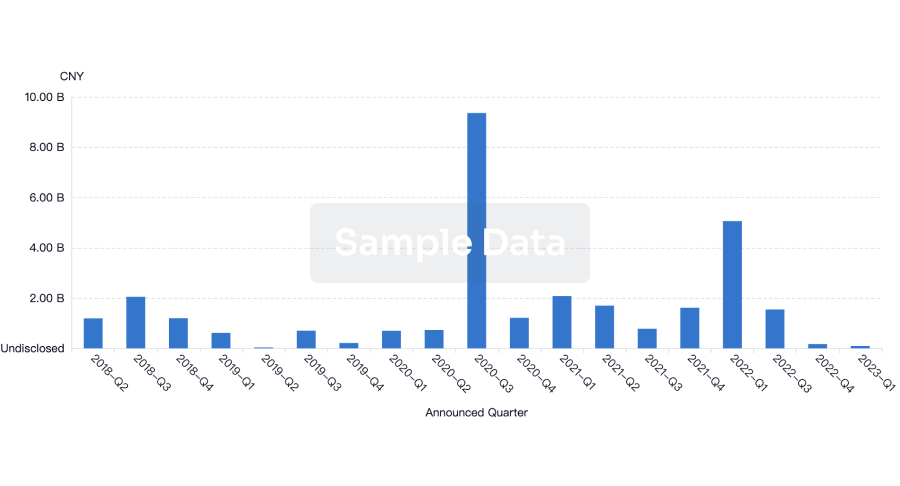
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
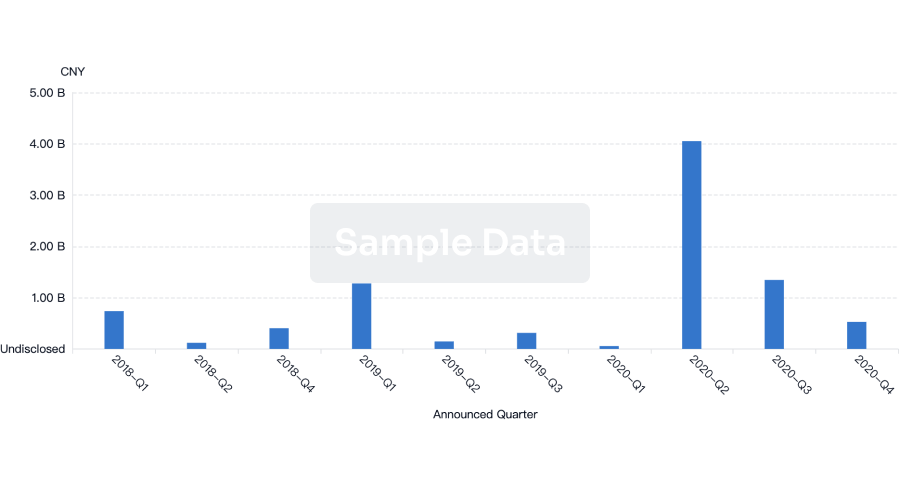
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free