Last update 28 Sep 2024

Orthopedic ONE
Last update 28 Sep 2024
Overview
Related
Randomized Controlled Trial of Home-based Physical Therapy Versus Outpatient Clinic-based Physical Therapy Following Primary Anterior Total Hip Arthroplasty
The Use of Teriparatide as an Adjunctive Therapy for the Treatment of Jones Fractures
100 Clinical Results associated with Orthopedic ONE
Login to view more data
Login to view more data
01 Oct 2014The Journal of bone and joint surgery. American volumeQ2 · MEDICINE
Associations Between Preoperative Physical Therapy and Post-Acute Care Utilization Patterns and Cost in Total Joint Replacement
Q2 · MEDICINE
Article
Author: Vogel, Karen ; Granata, Jaymes ; Ruhil, Anirudh V S ; Wasielewski, Ray ; Snow, Richard ; McShane, Michael
BACKGROUND:
Health-care costs following acute hospital care have been identified as a major contributor to regional variation in Medicare spending. This study investigated the associations of preoperative physical therapy and post-acute care resource use and its effect on the total cost of care during primary hip or knee arthroplasty.
METHODS:
Historical claims data were analyzed using the Centers for Medicare & Medicaid Services Limited Data Set files for Diagnosis Related Group 470. Analysis included descriptive statistics of patient demographic characteristics, comorbidities, procedures, and post-acute care utilization patterns, which included skilled nursing facility, home health agency, or inpatient rehabilitation facility, during the ninety-day period after a surgical hospitalization. To evaluate the associations, we used bivariate and multivariate techniques focused on post-acute care use and total episode-of-care costs.
RESULTS:
The Limited Data Set provided 4733 index hip or knee replacement cases for analysis within the thirty-nine-county Medicare hospital referral cluster. Post-acute care utilization was a significant variable in the total cost of care for the ninety-day episode. Overall, 77.0% of patients used post-acute care services after surgery. Post-acute care utilization decreased if preoperative physical therapy was used, with only 54.2% of the preoperative physical therapy cohort using post-acute care services. However, 79.7% of the non-preoperative physical therapy cohort used post-acute care services. After adjusting for demographic characteristics and comorbidities, the use of preoperative physical therapy was associated with a significant 29% reduction in post-acute care use, including an $871 reduction of episode payment driven largely by a reduction in payments for skilled nursing facility ($1093), home health agency ($527), and inpatient rehabilitation ($172).
CONCLUSIONS:
The use of preoperative physical therapy was associated with a 29% decrease in the use of any post-acute care services. This association was sustained after adjusting for comorbidities, demographic characteristics, and procedural variables.
CLINICAL RELEVANCE:
Health-care providers can use this methodology to achieve an integrative, cost-effective, patient care pathway using preoperative physical therapy.
01 Sep 2013Orthopedic nursingQ4 · MEDICINE
Q4 · MEDICINE
Article
Author: Latshaw, James C ; Price, Matthew C ; Horn, Pamela L
Proximal humerus fractures are among the most common fractures associated with osteoporosis. With an aging population, incidence of these fractures will only increase. The proximal humerus not only forms the lateral portion of the shoulder articulation but also has significant associations with musculoskeletal and neurovascular structures. As a result, fractures of the proximal humerus can significantly impact not only the function of the shoulder joint, but the health and function of the entire upper extremity as well. Understanding of these fractures, the management options, and associated nursing care, can help reduce morbidity rate and improve functional outcomes.
25 Jul 2012JBJS case connector
A Sixty-One-Year-Old Woman with Ischemia After Total Knee Arthroplasty
Article
Author: Wilmoth, Jill C ; McShane, Michael A ; Ng, Vincent Y
Arterial complications after total knee arthroplasty are rare, but potentially devastating. Most cases are attributable to predisposing patient risk factors and iatrogenic trauma or manipulation1. Numerous causes, such as thrombosis, vessel severance, aneurysm, and plaque embolization, have been reported in the literature1-4, and the anatomic relationships in the popliteal fossa have been well-described5. We present a case of acute ischemia after total knee arthroplasty associated with position-dependent occlusion of the popliteal artery. The contributing factors included a common underlying patient condition and a frequently used femoral component design. Orthopaedic surgeons that perform total knee arthroplasty regularly should be cognizant of the hallmark presentation of this complication, the appropriate clinical workup, and the optimal treatment options. The patient was informed that data concerning the case would be submitted for publication, and she provided consent.
A sixty-one-year-old woman presented with acute right leg ischemia in the postoperative recovery unit after routine cemented total knee arthroplasty for osteoarthritis. She had symptoms of marked pain and weakness throughout the leg. Surgery had been performed via a standard medial parapatellar approach with a tourniquet in place. An LPS-Flex Fixed Bearing implant system (Zimmer, Warsaw, Indiana) with a size 5 tibial baseplate, 29-mm patella, 14-mm polyethylene insert, and size F gender-specific femoral component had been used. Preoperative templating for size and alignment as well as intraoperative bone resection had been facilitated by the Patient Specific Instrumentation (PSI) system (Zimmer). The posterior osteophytes had been removed to achieve full knee extension, and soft-tissue balancing had included subperiosteal elevation of the posterior oblique ligament, deep medial collateral ligament, and semimembranosus tendon insertion.
The patient’s medical history included hypertension, coronary artery disease, and carotid artery disease. She denied exertional chest pain or lower-extremity claudication. The remainder of the history was noncontributory. …
13 Apr 2023
100 Deals associated with Orthopedic ONE
Login to view more data
100 Translational Medicine associated with Orthopedic ONE
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Oct 2024
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
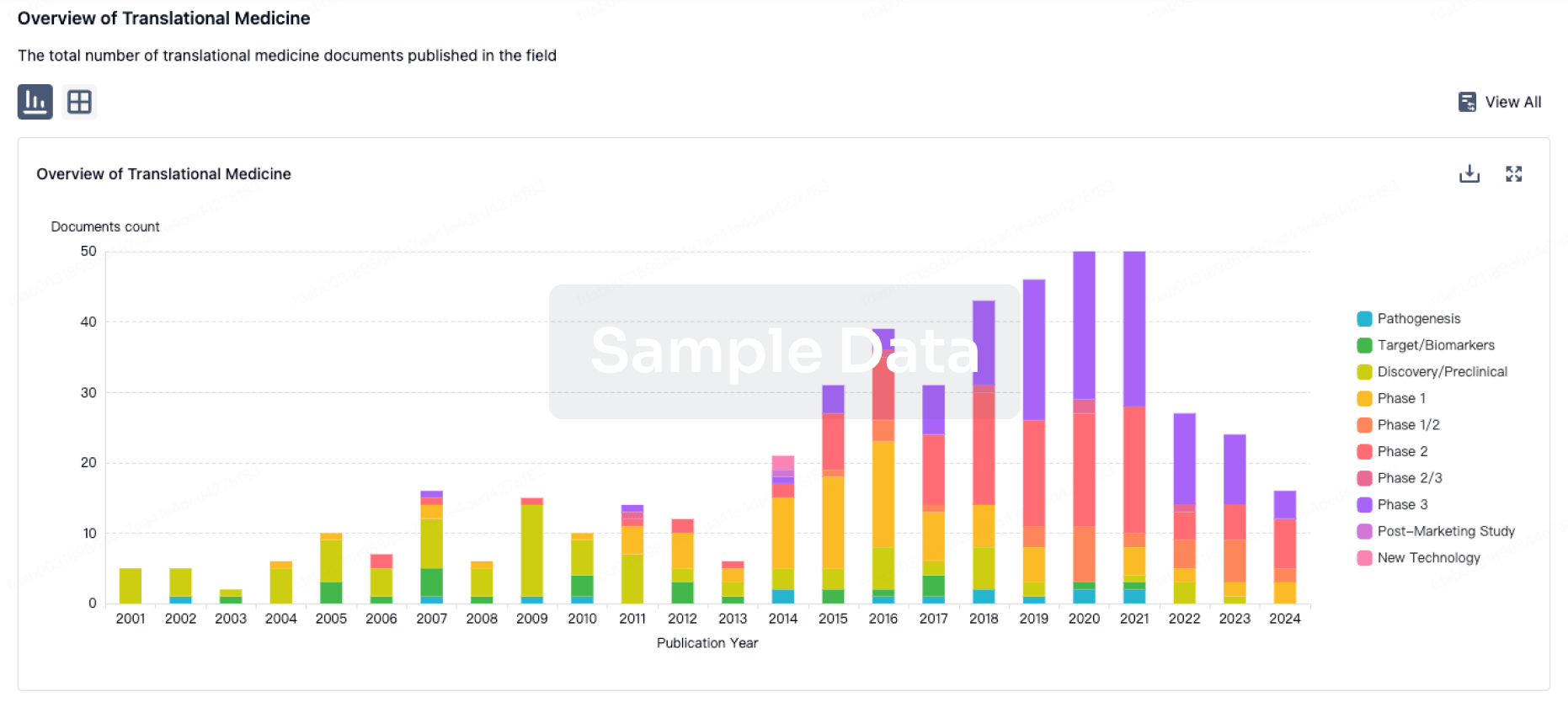
Translational Medicine
Boost your research with our translational medicine data.
login
or
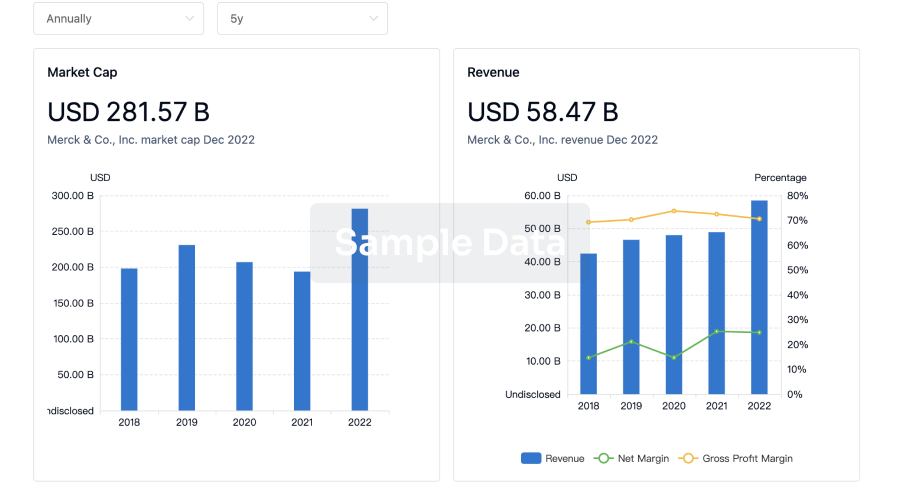
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free