Last update 06 Oct 2024
National Cardiology Hospital
Hospital|
Bulgaria
Last update 06 Oct 2024
Overview
Related
Echocardiographic Assessment and CLInical imPlication of Functional tricuSpid rEgurgitation in Heart Failure With Reduced or Preserved Ejection Fraction (ECLIPSE-HF)
Strategy To Optimize PeriproCeduraL AnticOagulation in Structural Transseptal Interventions (STOP CLOT Trial) - STOP CLOT
Morbidity research of traditional Chinese medicine patterns as related to conventional medicine diseases: An observational study on systemic arterial hypertension
100 Clinical Results associated with National Cardiology Hospital
Login to view more data
Login to view more data
25 Apr 2024The New England journal of medicine
Empagliflozin after Acute Myocardial Infarction
Article
Author: Jones, W Schuyler ; Zwiener, Isabella ; Mattheus, Michaela ; Gotcheva, Nina ; Udell, Jacob A ; Amir, Offer ; Sumin, Mikhail ; Anker, Stefan D ; Butler, Javed ; Schou, Morten ; Steg, P Gabriel ; Bayes-Genis, Antoni ; van der Meer, Peter ; Petrie, Mark C ; Jeong, Myung Ho ; Rossello, Xavier ; Brueckmann, Martina ; Chopra, Vijay K ; Vinereanu, Dragos ; Goodman, Shaun G ; Ge, Junbo ; Bahit, M Cecilia ; Goto, Shinya ; Hernandez, Adrian F ; Januzzi, James L ; Parkhomenko, Alexander ; Chen, Yundai ; Figtree, Gemma ; Jamal, Waheed ; Szachniewicz, Joanna ; Simic, Dragan ; Parikh, Puja B ; Bhatt, Deepak L ; Harrington, Josephine ; Lopatin, Yuri ; Zieroth, Shelley ; Ponikowski, Piotr ; Bauersachs, Johann ; Merkely, Béla ; Gasior, Tomasz ; Lopes, Renato D
BACKGROUND:
Empagliflozin improves cardiovascular outcomes in patients with heart failure, patients with type 2 diabetes who are at high cardiovascular risk, and patients with chronic kidney disease. The safety and efficacy of empagliflozin in patients who have had acute myocardial infarction are unknown.
METHODS:
In this event-driven, double-blind, randomized, placebo-controlled trial, we assigned, in a 1:1 ratio, patients who had been hospitalized for acute myocardial infarction and were at risk for heart failure to receive empagliflozin at a dose of 10 mg daily or placebo in addition to standard care within 14 days after admission. The primary end point was a composite of hospitalization for heart failure or death from any cause as assessed in a time-to-first-event analysis.
RESULTS:
A total of 3260 patients were assigned to receive empagliflozin and 3262 to receive placebo. During a median follow-up of 17.9 months, a first hospitalization for heart failure or death from any cause occurred in 267 patients (8.2%) in the empagliflozin group and in 298 patients (9.1%) in the placebo group, with incidence rates of 5.9 and 6.6 events, respectively, per 100 patient-years (hazard ratio, 0.90; 95% confidence interval [CI], 0.76 to 1.06; P = 0.21). With respect to the individual components of the primary end point, a first hospitalization for heart failure occurred in 118 patients (3.6%) in the empagliflozin group and in 153 patients (4.7%) in the placebo group (hazard ratio, 0.77; 95% CI, 0.60 to 0.98), and death from any cause occurred in 169 (5.2%) and 178 (5.5%), respectively (hazard ratio, 0.96; 95% CI, 0.78 to 1.19). Adverse events were consistent with the known safety profile of empagliflozin and were similar in the two trial groups.
CONCLUSIONS:
Among patients at increased risk for heart failure after acute myocardial infarction, treatment with empagliflozin did not lead to a significantly lower risk of a first hospitalization for heart failure or death from any cause than placebo. (Funded by Boehringer Ingelheim and Eli Lilly; EMPACT-MI ClinicalTrials.gov number, NCT04509674.).
14 Jul 2023Diagnostics (Basel, Switzerland)
Surgical Anatomy of the Liver-Significance in Ovarian Cancer Surgery.
Review
Author: Selçuk, Ilker ; Dineva, Svetla ; Watrowski, Rafał ; Kornovski, Yavor ; Slavchev, Stanislav ; Dzhenkov, Deyan ; Kostov, Stoyan ; Yordanov, Angel ; Ivanova, Yonka
INTRODUCTION:
Ovarian cancer is the leading cause of death among all gynecological malignancies. Most patients present with an advanced stage of the disease. The routes of spread in ovarian cancer include peritoneal dissemination, direct invasion, and lymphatic or hematogenous spread, with peritoneal and lymphatic spread being the most common among them. The flow direction of the peritoneal fluid makes the right subphrenic space a target site for peritoneal metastases, and the most frequently affected anatomical area in advanced cases is the right upper quadrant. Complete cytoreduction with no macroscopically visible disease is the most important prognostic factor.
METHODS:
We reviewed published clinical anatomy reports associated with surgery of the liver in cases of advanced ovarian cancer.
RESULTS:
The disease could disseminate anatomical areas, where complex surgery is required-Morrison's pouch, the liver surface, or porta hepatis. The aim of the present article is to emphasize and delineate the gross anatomy of the liver and its surgical application for oncogynecologists. Moreover, the association between the gross and microscopic anatomy of the liver is discussed. Additionally, the vascular supply and variations of the liver are clearly described.
CONCLUSIONS:
Oncogynecologists performing liver mobilization, diaphragmatic stripping, and porta hepatis dissection must have a thorough knowledge of liver anatomy, including morphology, variations, functional status, potential diagnostic imaging mistakes, and anatomical limits of dissection.
01 Jul 2023Radiology case reports
Disorder of sexual development, urinary bladder duplication, pancake kidney and neural tube defect.
Author: Landzhov, Boycho ; Gaydarski, Lyubomir ; Dineva, Svetla
Congenital malformations of the urogenital system with fully developed duplications, such as urinary bladder, are sporadic. They are often present in the setting of endogenous molecular disbalance, such as steroid metabolism disturbances. Other rare manifestations of hormonal disbalance present as intersex conditions in which the individual has karyotype-specific internal genital organs with opposite-sex signs of the external genitalia, known as ambiguous genitalia. Congenital variations and malformations are often fully recognized and understood during radiological exams. Herein we present a unique case of a 2-month-old baby with female chromosomal sex and ambiguous genitalia together with the manifestation of several anatomical malformations: urinary bladder duplication in the coronal plane, pancake kidney with supernumerary renal arteries, 2 ureters and neural tube defect. Despite their low incidence rate, knowledge of such malformations is paramount for correct diagnosis and treatment in such cases.

100 Deals associated with National Cardiology Hospital
Login to view more data
100 Translational Medicine associated with National Cardiology Hospital
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Oct 2024
No data posted
Login to keep update
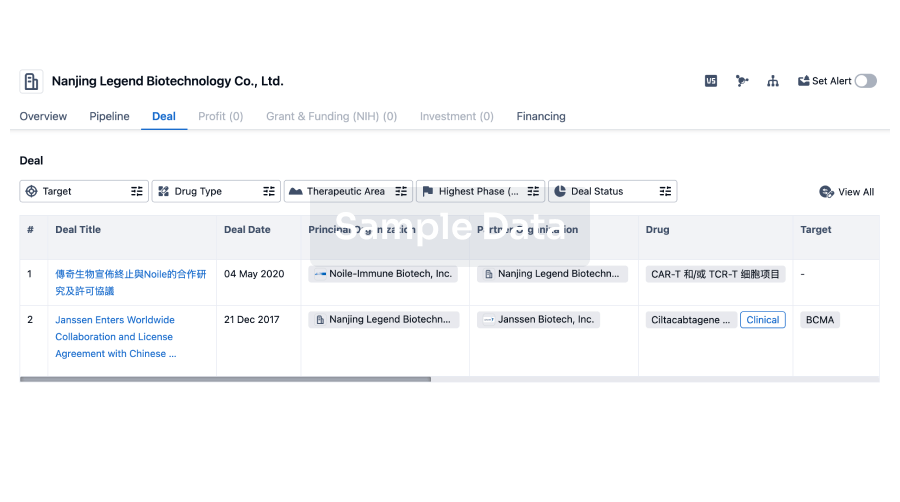
Deal
Boost your decision using our deal data.
login
or
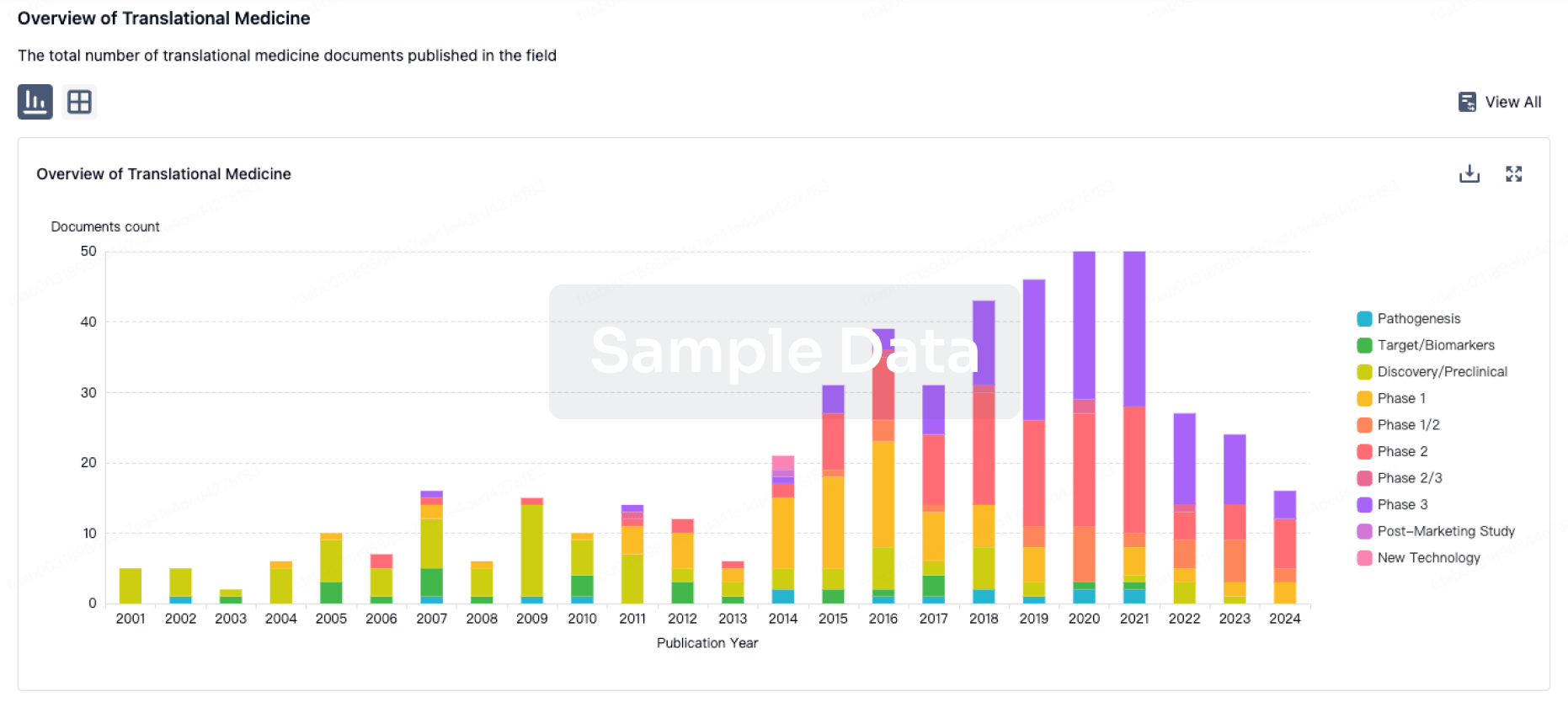
Translational Medicine
Boost your research with our translational medicine data.
login
or
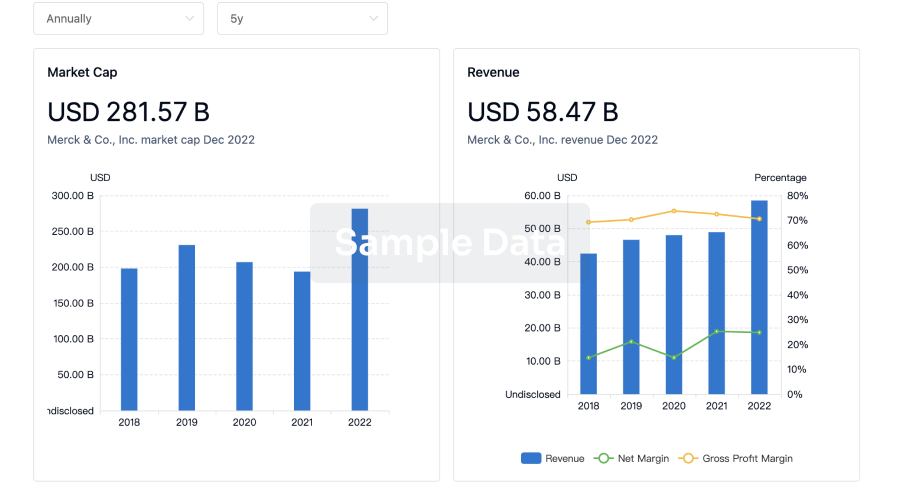
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free