Request Demo
Last update 23 Jan 2025
Breath Therapeutics, Inc.
Private Company|
United States
Private Company|
United States
Last update 23 Jan 2025
Overview
Related
1
Clinical Trials associated with Breath Therapeutics, Inc.EUCTR2019-000718-13-ES
A Phase IIa Multi-Center, Randomized, Single-Blind Safety Study of Liposomal Cyclosporine A to Treat Bronchiolitis Obliterans Syndrome Following Allogeneic Hematopoietic Stem Cell Transplantation. - BOSTON-4
Start Date27 Nov 2019 |
Sponsor / Collaborator |
100 Clinical Results associated with Breath Therapeutics, Inc.
Login to view more data
0 Patents (Medical) associated with Breath Therapeutics, Inc.
Login to view more data
4
Literatures (Medical) associated with Breath Therapeutics, Inc.01 May 2021·TP23. TP023 LUNG TRANSPLANT: OUTCOME PREDICTORS AND THERAPEUTIC OPTIONS
Study Design of Two Phase III, Prospective, Multicenter, Randomized, Controlled Clinical Trials Evaluating the Efficacy and Safety of Liposomal Cyclosporin A for Inhalation(L-CsA-i) in Patients with Bronchiolitis Obliterans Syndrome Post Single- (BOSTON-1) or Double- (BOSTON-2) Lung Transplantation
Author: Cuomo, D. ; Hachem, R.R. ; Prante Fernandes, S. ; McGrain, J. ; Boerner, G. ; Monforte Torres, V.
01 Jan 2020·Journal of Cystic Fibrosis
Antisense oligonucleotide eluforsen is safe and improves respiratory symptoms in F508DEL cystic fibrosis
Article
Author: Drevinek, Pavel ; Paquette-Lamontagne, Nicolas ; Elborn, J Stuart ; Cipolli, Marco ; Pressler, Tacjana ; den Hollander, Wilhelmina ; Tomkinson, Nigel ; De Boeck, Kris ; Montgomery, Sonya ; Henig, Noreen ; Schwarz, Carsten ; Bouisset, Florilene ; Boff, Marie ; Perquin, Jaakko
13 Nov 2019·Blood
Economic Burden of Bronchiolitis Obliterans Syndrome (BOS) Following Allogeneic Hematopoietic Stem Cell Transplant (alloHSCT) in Patients with Commercial Insurance in the United States
Author: Healey, Bridget ; Cyr, Philip ; Batt, Katharine ; Henig, Noreen Roth ; Sacks, Naomi
100 Deals associated with Breath Therapeutics, Inc.
Login to view more data
100 Translational Medicine associated with Breath Therapeutics, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 02 Feb 2025
No data posted
Login to keep update
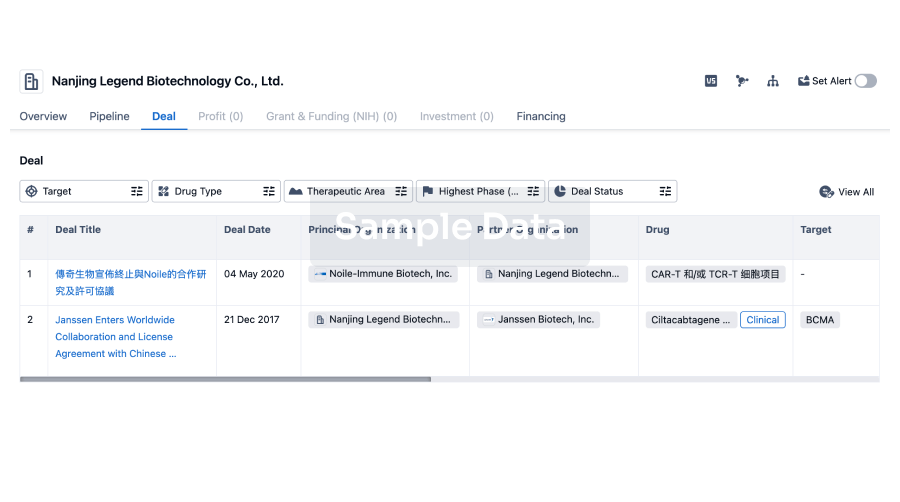
Deal
Boost your decision using our deal data.
login
or
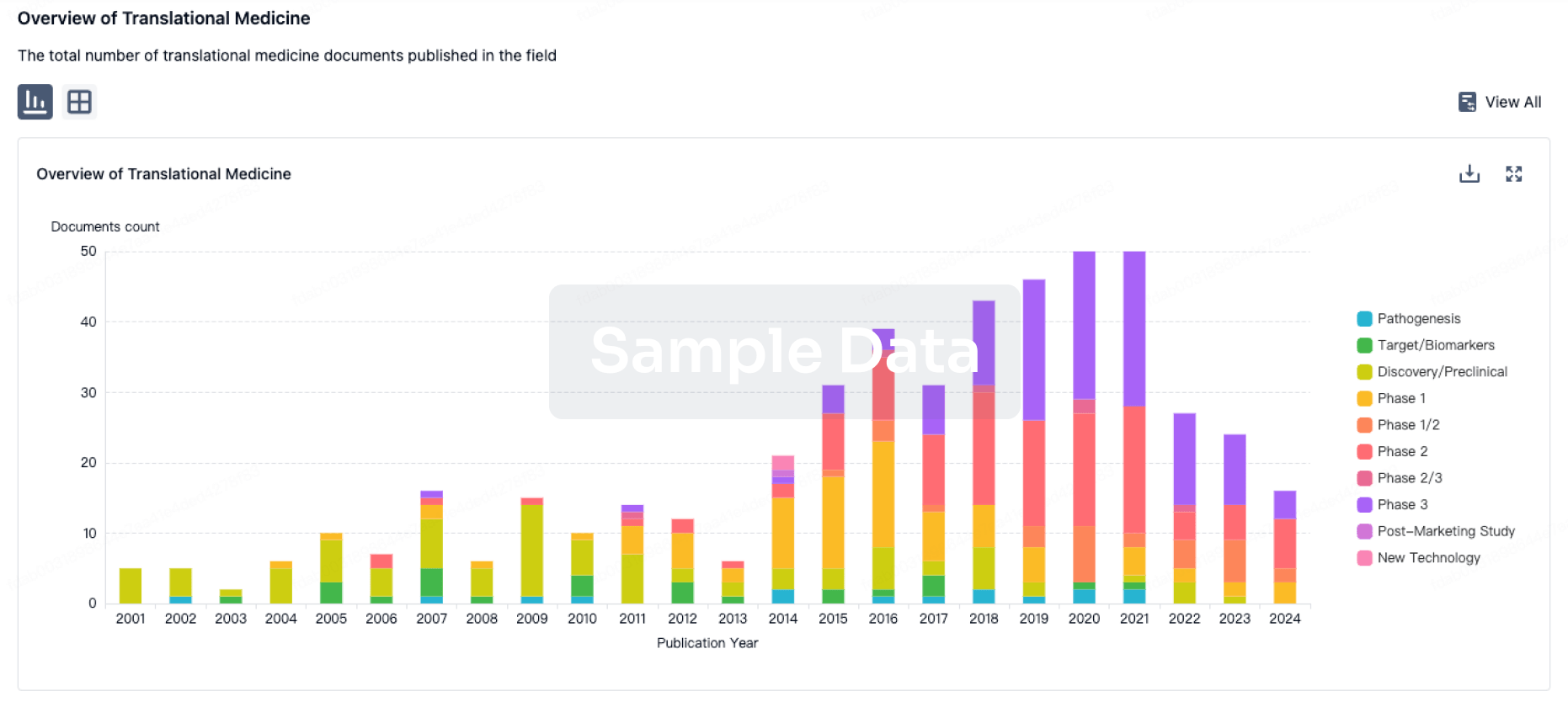
Translational Medicine
Boost your research with our translational medicine data.
login
or
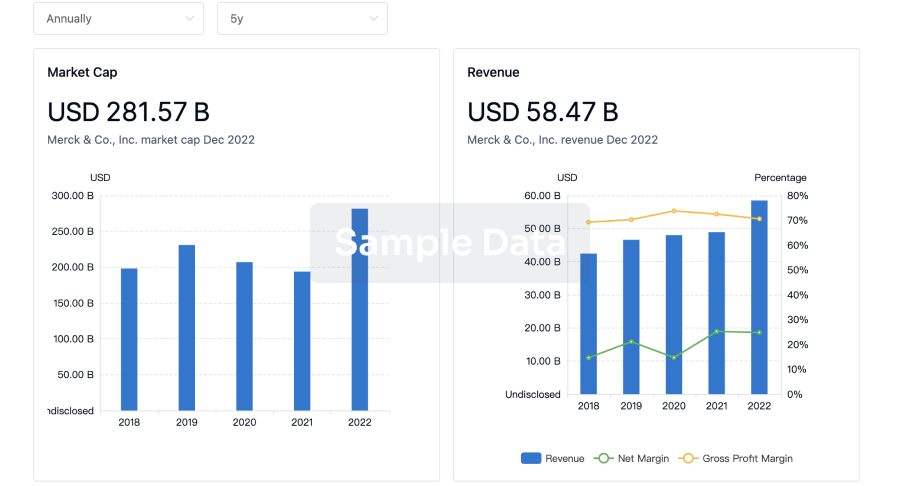
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
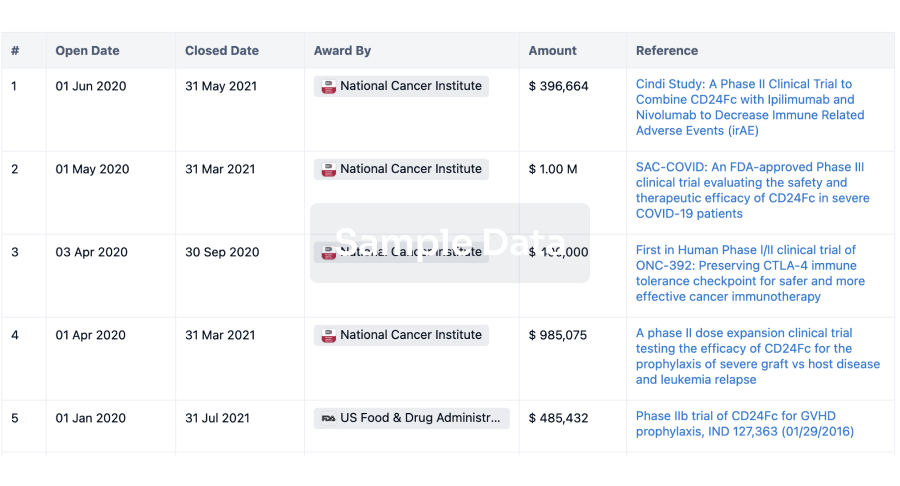
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
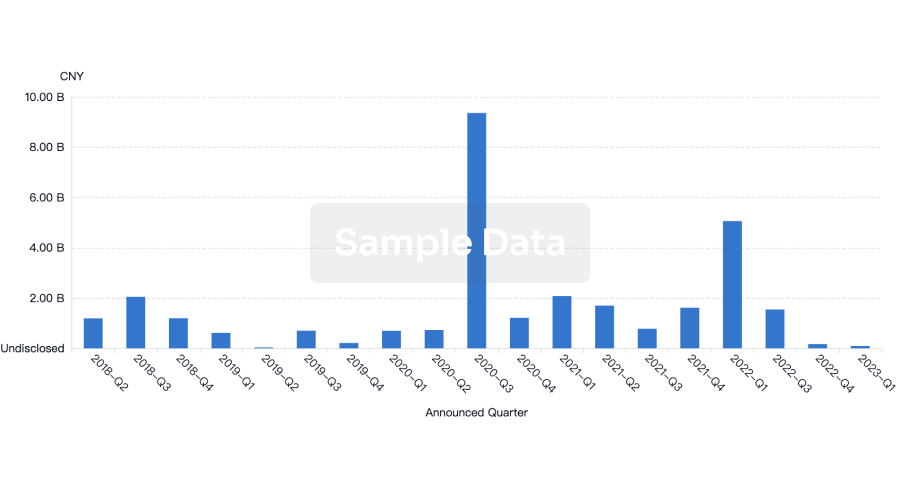
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
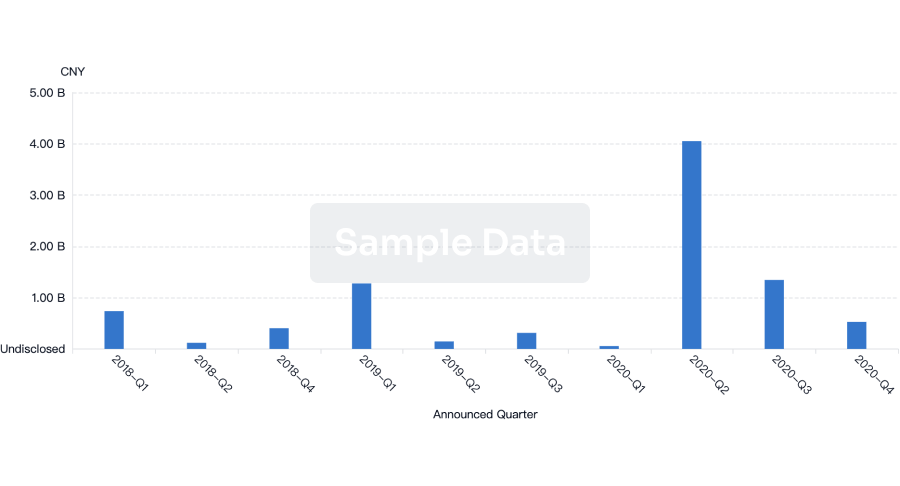
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free