Iron Deficiency in Pediatric Heart Surgery: Impact on Anemia, Transfusion and Complications, a Retrospective Cohort Study
The prevalence of iron deficiency in pediatric cardiac surgery patients is not very well known. Iron deficiency can lead to anemia, higher transfusion rates and possibly higher complication rates. In this retrospective study, the iron status of all patients undergoing pediatric cardiac surgery at our institution between January 2019 and december 2023 will be analyzed. Together with iron status, transfusion requirements as well as complications will be recorded. Iron status will be reported with descriptive statistics, patients with or without iron deficiency will be compared using non-parametric tests.
Prospective Unblinded Randomized Controlled Study Assessing the Physiologically Based Cord Clamping on Ventilation Duration in Moderate and Late Preterm
Before birth, the baby's lungs are filled with fluid and babies do not use the lungs to breathe, as the oxygen comes from the placenta. As delivery approaches, the lungs begin to absorb the fluid. After vaginal delivery, the umbilical cord is clamped and cut after a delay that allows some of the blood in the umbilical cord and placenta to flow back into the baby. Meanwhile, as the baby breathes for the first time, the lungs fill with air and more fluid is pushed out. However, it does not always work out that way.
A baby born prematurely may have breathing problems because of extra fluid staying in the lungs related to the immaturity of the lung structure. Thus, the baby must breathe quicker and harder to get enough oxygen enter into the lungs. The newborn is separated from the mother to provide emergency respiratory support. Although the baby is usually getting better within one or two days, the treatment requires close monitoring, breathing help, and nutritional help as the baby is too tired to suck and swallow milk. Sometimes, the baby cannot recover well and show greater trouble breathing needing intensive care. This further separates the mother and her baby. A possible mean to help the baby to adapt better after a premature birth while staying close to the mother is to delay cord clamping when efficient breathing is established, either spontaneously or after receiving breathing help at birth. In this study, we intend to test this procedure in moderate or late preterm infants and see whether the technique helps the baby to better adapt after birth and to better initiate a deep bond with the mother.
Changes in Pulmonary Ventilation Distribution Assessed by EIT (Electrical Impedance Tomography) in Healthy Children Under General Anesthesia; a Pilot Study Comparing Mask Spontaneous Breathing and Laryngeal Mask Spontaneous Breathing With and Without Ventilatory Support
The incidence of atelectasis is high in patients undergoing general anesthesia. This may cause oxygenation impairment and further contribute to post-operative pulmonary complications. As important airway management devices for general anesthesia, few studies have compared the impact of laryngeal mask airway and spontaneous breathing on atelectasis. Through the study, the distribution of the pulmonary ventilation of children undergoing an elective and standard procedure in our center (H.U.D.E.R.F.) will be studied using electric impedance tomography.
Children from 1 year-old to 6-year-old, ASA physical status I or II who will undergo elective circumcisions under general anesthesia associated with regional anesthesia (Penile Block10) at the One Day Clinic of H.U.D.E.R.F. (Hôpital des Enfants Reine Fabiola - Brussels - Belgium).
Patients will be allocated to three different group in a ration of 1:1:1.
Group 1: spontaneous mask ventilation (20 patients).
Group 2: spontaneous laryngeal mask (LMA) ventilation (20 patients).
Group 3: spontaneous-pressure support LMA ventilation (LMA SV-PS) (20 patients).
Standard monitoring for the inductions of the anesthesia will include non-invasive blood pressure (NIBP), pulse oximetry (SpO2), Electrocardiogram (ECG), End-Tidal CO2 (EtCO2), End Tidal Sevoflurane concentration (EtSev %), inspired fraction of oxygen (FiO2), body temperature (rectal thermometer).
Induction is based as well on the local routine protocols using an inhalation induction of the patient with Sevoflurane (Fet of 6-8%) and a recommended FiO2 from 80-90% maximum until the stabilization of the induction. Then the FiO2 will be decreased at least under 40% and Sevoflurane adapted to the need of the deepness of the anesthesia (both at the discretion of the anesthesiologist in charge of the patient).
Depending on the randomization, the patient will undergo the surgery either with spontaneous face mask ventilation (group 1), LMA spontaneous ventilation (group 2), or LMA SV-PS (group 3) (during which the pressure support will be adapted at the discretion of the anesthesiologist but with a tidal volume included in the range of 6-10ml/kg).
Electrical impedance tomography measurements:
The effects of the spontaneous breathing (mask ventilation or LMA) or the pressure support ventilation (LMA SV-PS) on atelectasis formations and the distribution of the ventilation will be assessed using electrical impedance tomography.
The device used during the study will be the "PulmoVista 500"; it will be provided by Dräger (Lübeck, Germany) free of charge and without any obligation or results/conclusions requested by Dräger. The device is approved CE (European regulation) and will be used in the conditions for which it has been designed.
A reusable belt with 16 evenly spaced electrodes will be placed around the chest of each patient included in the study between the 4th and 6th ribs as recommended by Dräger.
The EIT measurements will be taken of 4 different moments:
T1: Before induction of the anesthesia in the preoperatory waiting room (and at least 30 min after the premedication).
T2: After the induction of anesthesia (GA and penile block), just before the beginning of the surgical procedure.
T3: After the end of the surgical procedure, just before discontinuing the general anesthesia.
T4: Before the discharge of the PACU.
100 Clinical Results associated with Queen Fabiola Children's University Hospital
0 Patents (Medical) associated with Queen Fabiola Children's University Hospital
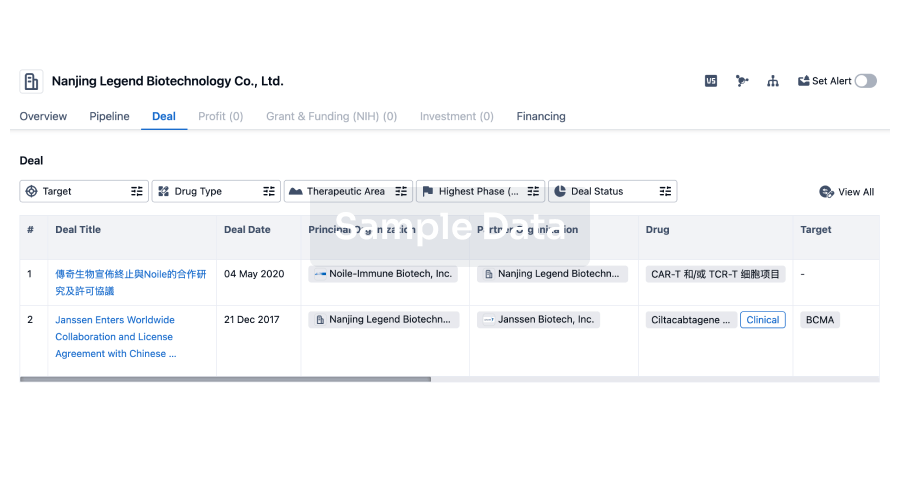
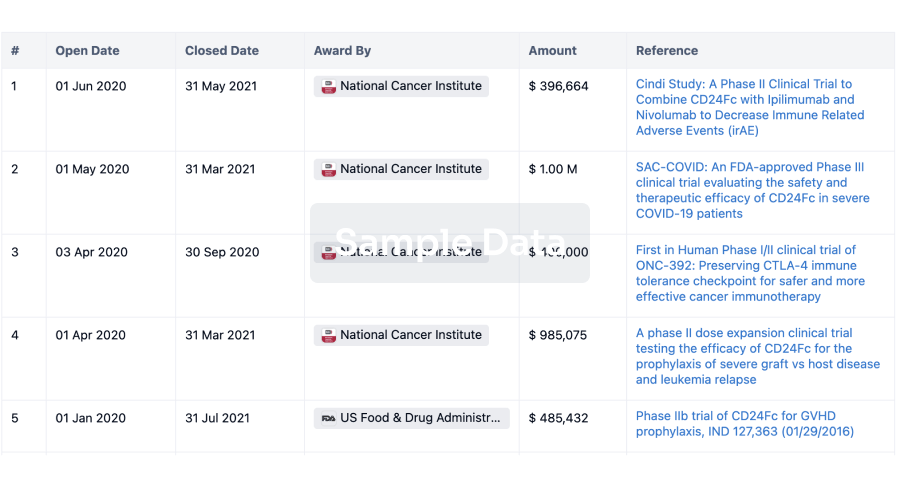
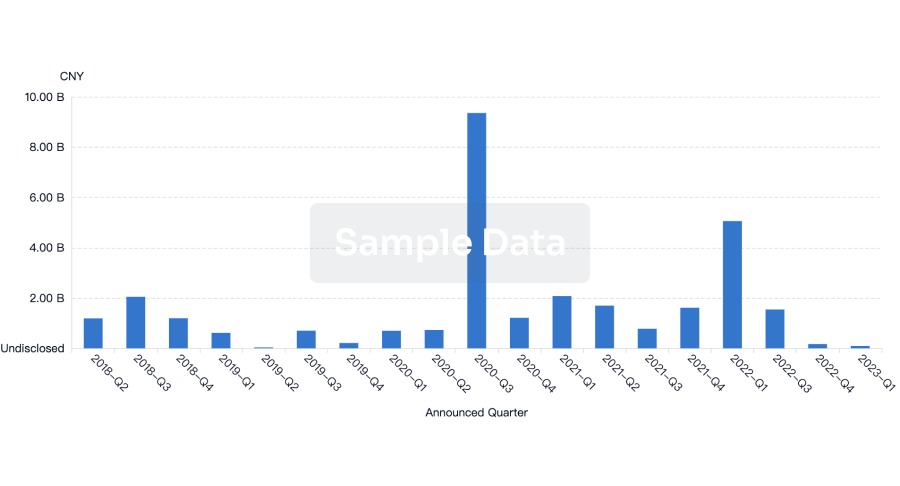
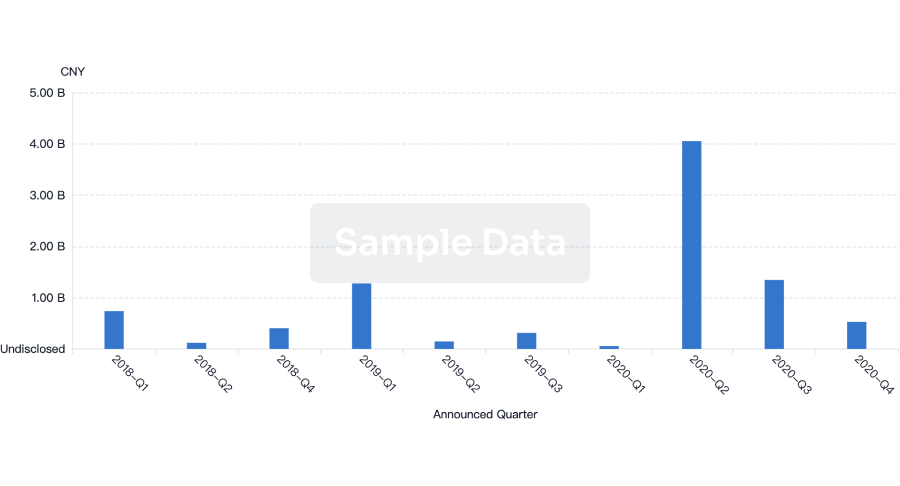
100 Deals associated with Queen Fabiola Children's University Hospital
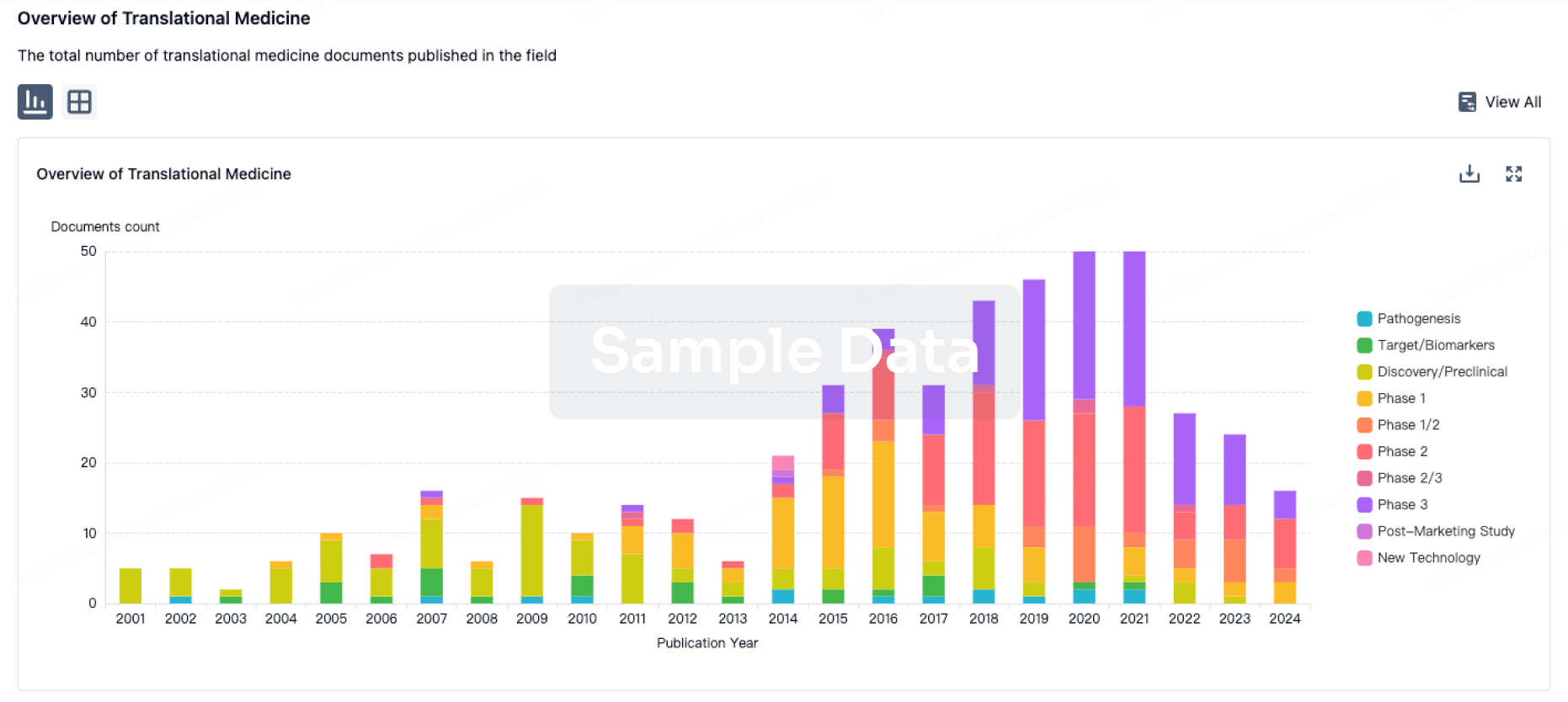
100 Translational Medicine associated with Queen Fabiola Children's University Hospital