Neurocrine Biosciences: After 30 years, a breakthrough in the development of CRF1 antagonists is imminent
Neurocrine Biosciences announced on its official website that the U.S. FDA has accepted two New Drug Applications (NDA) from the company, both with priority review designation, for the treatment of classic congenital adrenal hyperplasia (CAH) in children, adolescents, and adults using crinecerfont. If approved, crinecerfont will be the first new treatment option for CAH in 70 years and represents a novel therapeutic approach, offering a new treatment method for this rare and severe endocrine disorder.

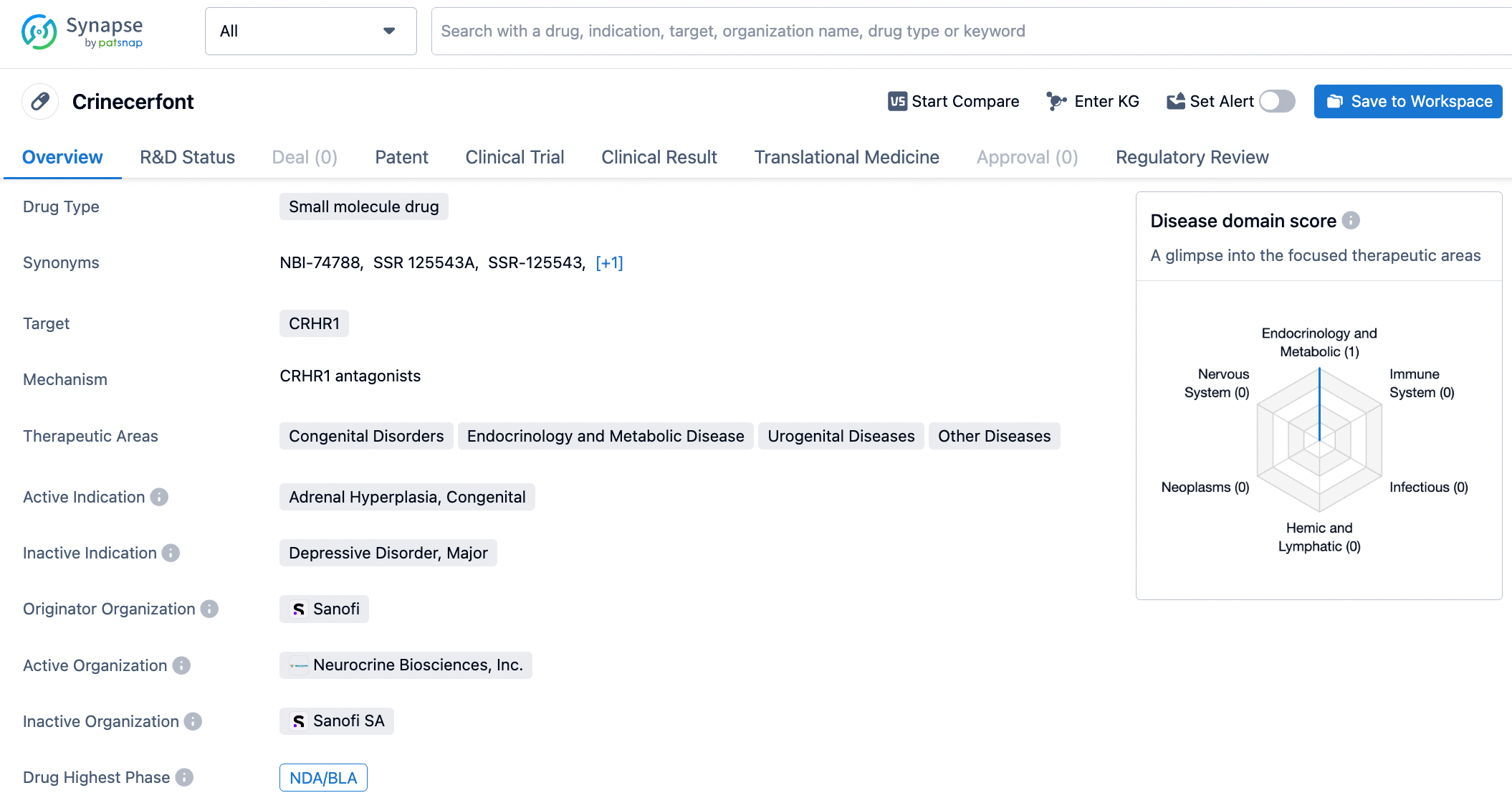
Crinecerfont is an orally administered selective corticotropin-releasing factor type 1 receptor (CRF1) antagonist currently under development for the treatment of congenital adrenal hyperplasia (CAH) caused by 21-hydroxylase deficiency. It works through a mechanism independent of glucocorticoids to reduce and control excessive levels of adrenocorticotropic hormone (ACTH) and adrenal androgens. Antagonizing CRF1 receptors in the pituitary gland has been shown to decrease ACTH levels, thereby reducing adrenal androgen production and potentially alleviating symptoms associated with CAH. Research data on crinecerfont indicates that lowering adrenal androgen levels can result in glucocorticoid dosages that are lower and more physiologically friendly, thereby potentially reducing complications in CAH patients due to exposure to higher-than-normal doses of glucocorticoids.
The NDAs submitted by Neurocrine Biosciences for crinecerfont include: (1) a capsule formulation (NDA# 218808) and (2) an oral solution formulation (NDA# 218820), both showcasing the primary efficacy and safety of crinecerfont for treating classic congenital adrenal hyperplasia (CAH).
Congenital Adrenal Hyperplasia
Congenital Adrenal Hyperplasia (CAH) is a genetic disorder characterized by enzyme deficiencies in the synthesis of adrenal corticosteroids, leading to insufficient production of cortisol and/or aldosterone. The most common form is 21-hydroxylase deficiency, accounting for 90%-95% of typical cases. This deficiency disrupts the conversion of adrenal precursors to cortisol, and in some cases, results in aldosterone deficiency, occasionally causing severe hyponatremia and hyperkalemia. The accumulated hormone precursors are diverted into androgen production, resulting in masculinization.
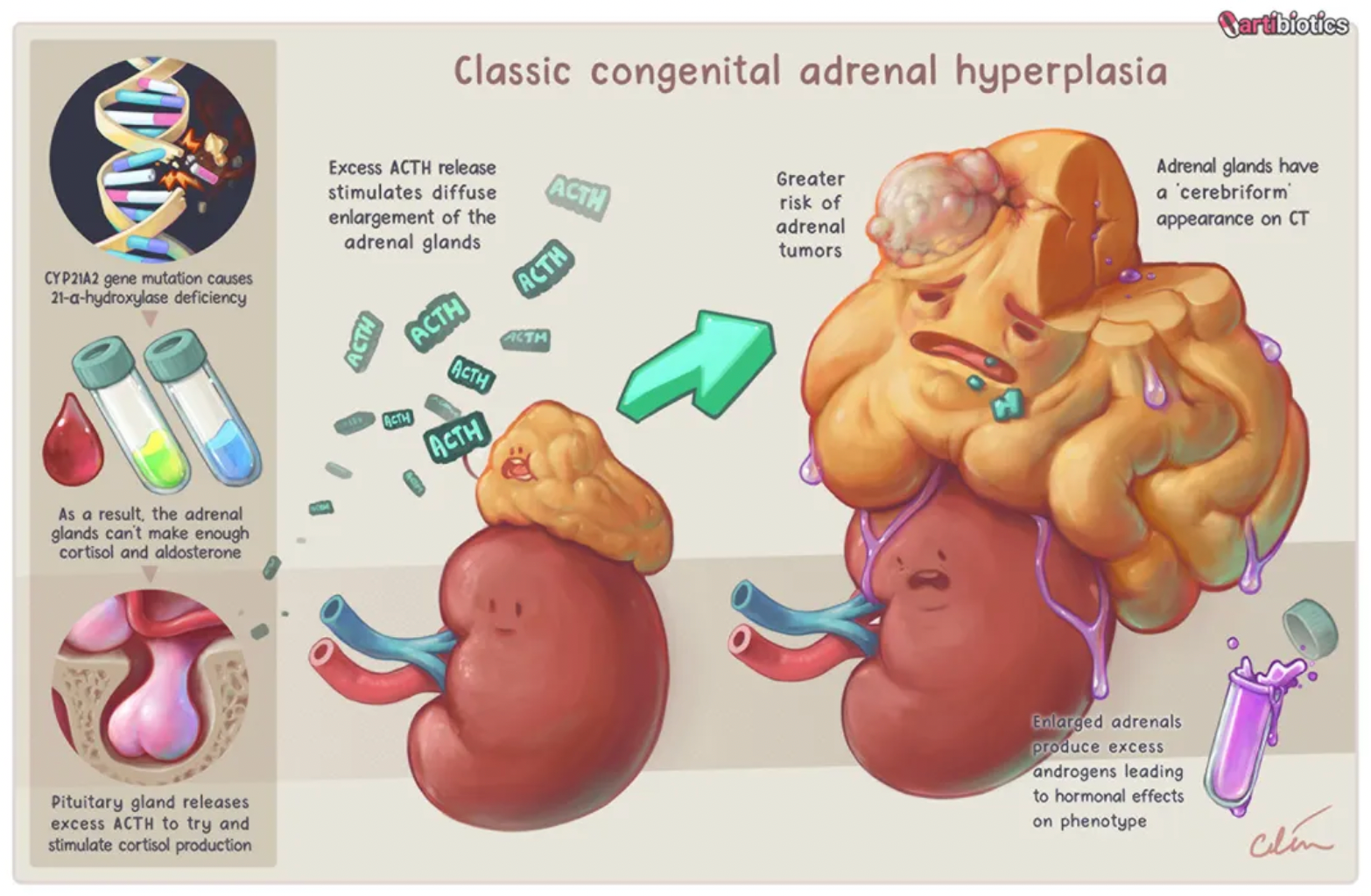
CAH is an autosomal recessive genetic condition, manifesting in individuals who are homozygous for the disease-causing gene (i.e., they have two copies), while heterozygous carriers (i.e., individuals with one copy of the gene) remain asymptomatic.
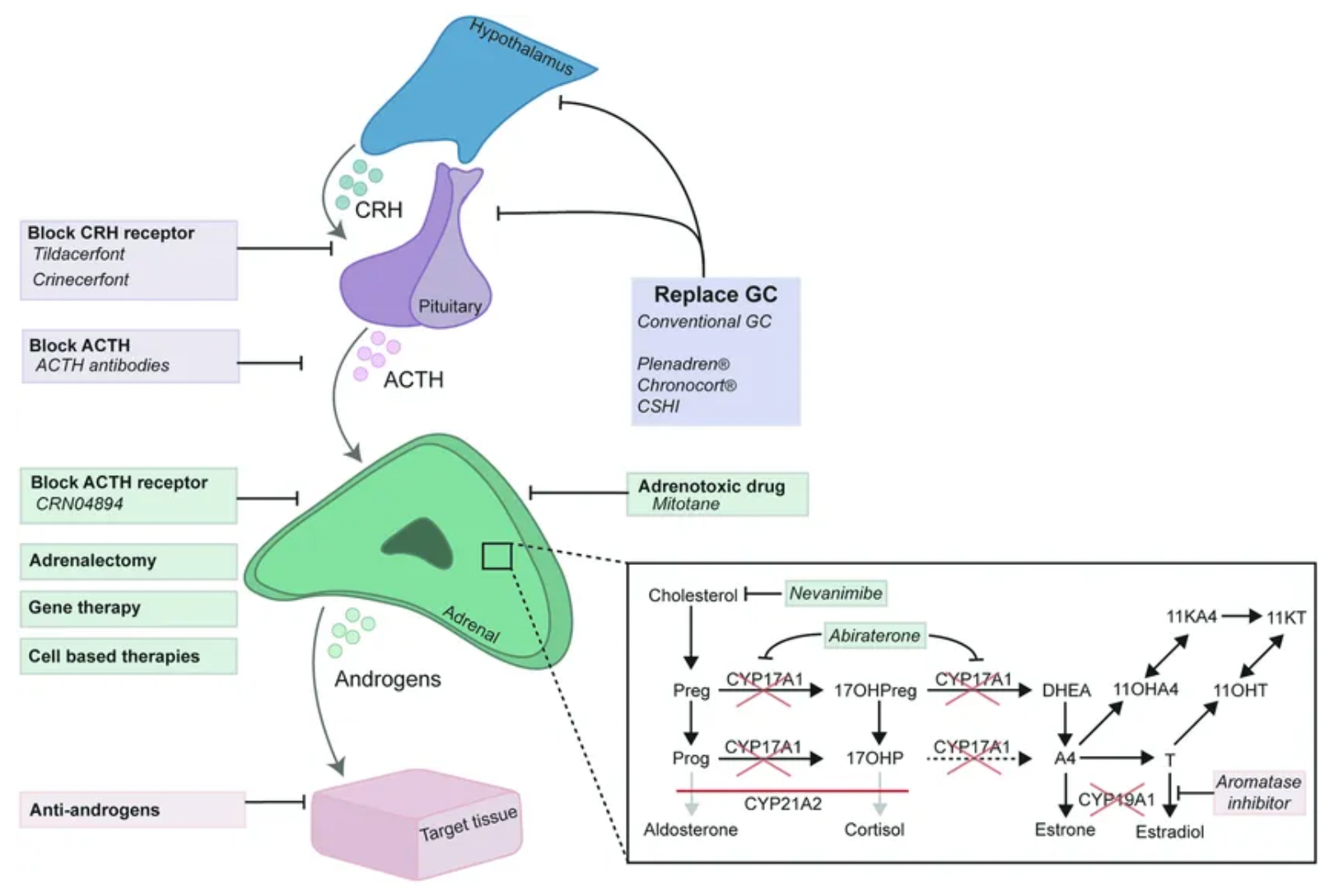
New treatments for 21-hydroxylase deficiency (21OHD) include the use of improved controlled-release formulations of hydrocortisone (e.g., Plenadren®, Chronocort®) or improved glucocorticoid (GC) delivery methods such as continuous subcutaneous hydrocortisone infusion (CSHI). These approaches are associated with more effective suppression of the hypothalamic-pituitary-adrenal (HPA) axis-driven adrenal androgen production. Moreover, blocking the production of adrenal androgens driven by the HPA axis can be further achieved through blocking corticotropin-releasing hormone (CRH) receptors (e.g., Tildacerfont, crinecerfont) or ACTH receptors. Adrenal androgen production can also be suppressed by adrenal steroidogenesis inhibitors (e.g., Nevanimibe, abiraterone acetate), adrenotoxic drugs (e.g., mitotane), or bilateral adrenalectomy. Inhibiting the aromatization of adrenal androgens may reduce the suppressive effect of estrogens on growth, while the (combined) use of anti-androgens may inhibit the effects of excess androgens. Gene and cell-based therapies are anticipated to restore the production of glucocorticoids and mineralocorticoids regulated by the HPA axis.
Crinecerfont (SSR-125543) is a selective CRF1 receptor antagonist originally developed by Sanofi. Early preclinical studies demonstrated that this molecule exhibited antidepressant effects in animal models.
However, subsequent clinical trials, specifically Phase II studies aimed at investigating its antidepressant efficacy, ended in failure.
Neurocrine Biosciences was also among the first companies globally to initiate the development of CRF1 receptor antagonists. The company partnered with Janssen Pharmaceuticals to develop CRF1 receptor antagonists for the treatment of a range of psychiatric, neurological, and gastrointestinal disorders including anxiety, depression, and irritable bowel syndrome. In 1996, Neurocrine Biosciences went public through an initial public offering and was listed on the NASDAQ stock exchange. Following the IPO, Neurocrine Biosciences embarked on clinical development collaborations with Eli Lilly and GlaxoSmithKline (GSK) to explore CRF antagonists (such as NBI-34041) for the treatment of obesity, Alzheimer's disease, and as antidepressants. Nonetheless, many of these clinical developments also ended in failure.
In 2015, Neurocrine Biosciences disclosed a patent where CRF1 receptor antagonists were used to treat congenital adrenal hyperplasia (CAH). The company demonstrated the potential of CRF1 receptor antagonists to directly inhibit the release of ACTH in patients with CAH, which in turn could reduce the physiological dosage of hydrocortisone necessary, normalize androgen production, and thereby reduce treatment-related side effects.
It is worth mentioning that the method cited in the patent claims involves several CRF1 antagonist products reported on the market, including the original research products NBI-30775 and NBI-34041, as well as SSR-126374, SSR-125543, antalarmin, and DMP904.
After nearly 30 years, the company finally published the results of its research in a study titled "Phase 3 Trial of Crinecerfont in Adult Congenital Adrenal Hyperplasia" in The New England Journal of Medicine in 2024. This study demonstrated the efficacy and safety of the CRF1 antagonist product Crinecerfont, originally developed by Sanofi as SSR-125543, in the treatment of congenital adrenal hyperplasia.
The results show that among the total of 182 patients who participated in a 24-week trial, by week 24, there was a -27.3% change in the dosage of glucocorticoids in the Crinecerfont group compared to -10.3% in the placebo group. In the Crinecerfont group, 63% of patients reported glucocorticoid dosages within physiological levels, whereas in the placebo group, this proportion was 18%. Fatigue and headache were the most common adverse events in both trial groups. The conclusion indicates that in patients with congenital adrenal hyperplasia, the use of Crinecerfont as opposed to placebo resulted in a greater reduction in mean daily glucocorticoid dosage, including reductions to within the physiological range, following assessment of adrenal androgen levels.
How to obtain the latest research advancements in the field of biopharmaceuticals?
In the Synapse database, you can keep abreast of the latest research and development advances in drugs, targets, indications, organizations, etc., anywhere and anytime, on a daily or weekly basis. Click on the image below to embark on a brand new journey of drug discovery!